

New models and online calculator for predicting non-sentinel lymph node status in sentinel lymph node positive breast cancer patients
- PMID: 18315887
- PMCID: PMC2311316
- DOI: 10.1186/1471-2407-8-66
New models and online calculator for predicting non-sentinel lymph node status in sentinel lymph node positive breast cancer patients
Abstract
Background: Current practice is to perform a completion axillary lymph node dissection (ALND) for breast cancer patients with tumor-involved sentinel lymph nodes (SLNs), although fewer than half will have non-sentinel node (NSLN) metastasis. Our goal was to develop new models to quantify the risk of NSLN metastasis in SLN-positive patients and to compare predictive capabilities to another widely used model.
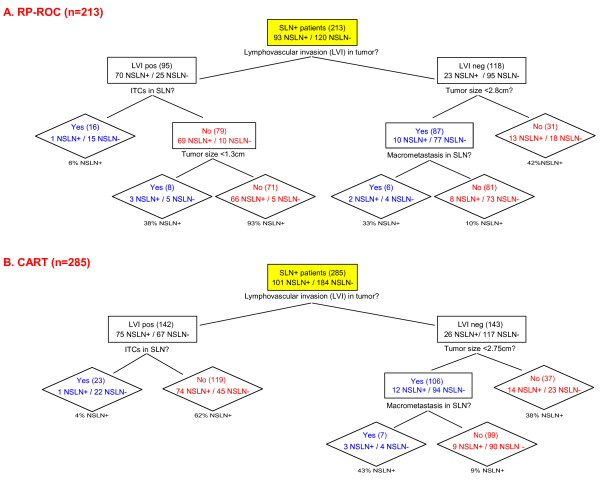
Methods: We constructed three models to predict NSLN status: recursive partitioning with receiver operating characteristic curves (RP-ROC), boosted Classification and Regression Trees (CART), and multivariate logistic regression (MLR) informed by CART. Data were compiled from a multicenter Northern California and Oregon database of 784 patients who prospectively underwent SLN biopsy and completion ALND. We compared the predictive abilities of our best model and the Memorial Sloan-Kettering Breast Cancer Nomogram (Nomogram) in our dataset and an independent dataset from Northwestern University.
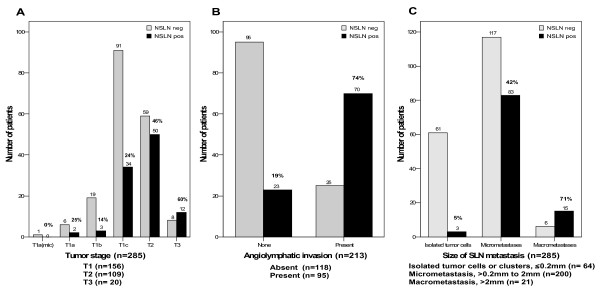
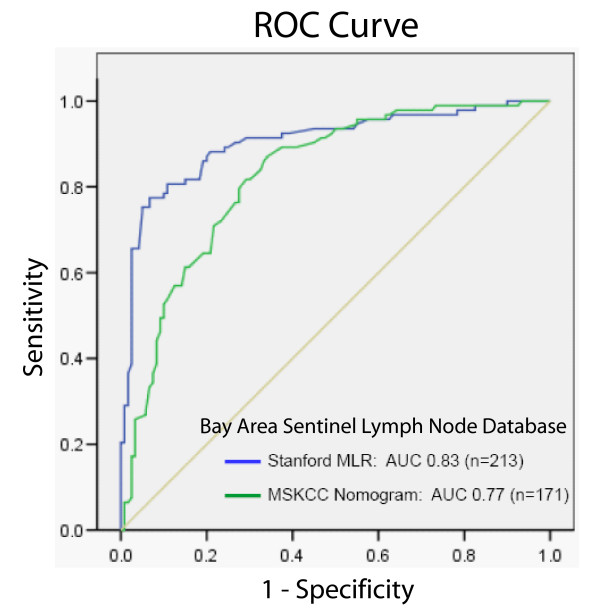
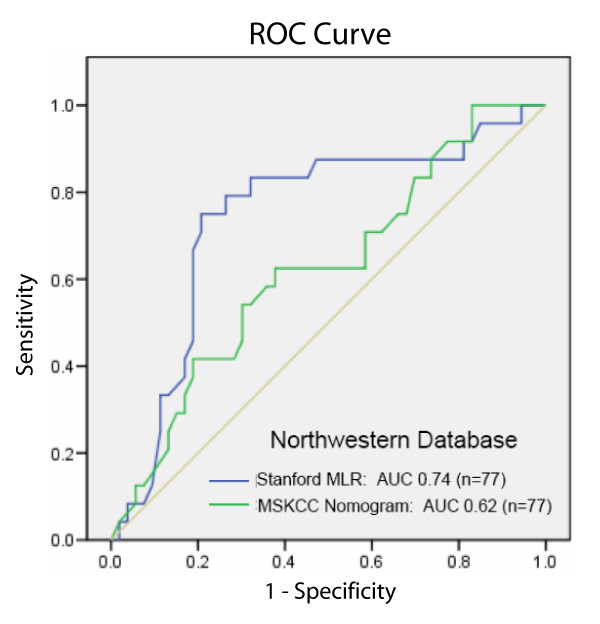
Results: 285 patients had positive SLNs, of which 213 had known angiolymphatic invasion status and 171 had complete pathologic data including hormone receptor status. 264 (93%) patients had limited SLN disease (micrometastasis, 70%, or isolated tumor cells, 23%). 101 (35%) of all SLN-positive patients had tumor-involved NSLNs. Three variables (tumor size, angiolymphatic invasion, and SLN metastasis size) predicted risk in all our models. RP-ROC and boosted CART stratified patients into four risk levels. MLR informed by CART was most accurate. Using two composite predictors calculated from three variables, MLR informed by CART was more accurate than the Nomogram computed using eight predictors. In our dataset, area under ROC curve (AUC) was 0.83/0.85 for MLR (n = 213/n = 171) and 0.77 for Nomogram (n = 171). When applied to an independent dataset (n = 77), AUC was 0.74 for our model and 0.62 for Nomogram. The composite predictors in our model were the product of angiolymphatic invasion and size of SLN metastasis, and the product of tumor size and square of SLN metastasis size.
Conclusion: We present a new model developed from a community-based SLN database that uses only three rather than eight variables to achieve higher accuracy than the Nomogram for predicting NSLN status in two different datasets.
Figures
References
-
- Lyman GH, Giuliano AE, Somerfield MR, Benson AB, 3rd, Bodurka DC, Burstein HJ, Cochran AJ, Cody HS, 3rd, Edge SB, Galper S, Hayman JA, Kim TY, Perkins CL, Podoloff DA, Sivasubramaniam VH, Turner RR, Wahl R, Weaver DL, Wolff AC, Winer EP. American Society of Clinical Oncology guideline recommendations for sentinel lymph node biopsy in early-stage breast cancer. J Clin Oncol. 2005;23:7703–7720. doi: 10.1200/JCO.2005.08.001. - DOI - PubMed
-
- Carlson RW, McCormick B. Update: NCCN breast cancer Clinical Practice Guidelines. J Natl Compr Canc Netw. 2005;3 Suppl 1:S7–11. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
