

A randomized, controlled trial of cognitive-behavioral therapy for augmenting pharmacotherapy in obsessive-compulsive disorder
- PMID: 18316422
- PMCID: PMC3945728
- DOI: 10.1176/appi.ajp.2007.07091440
A randomized, controlled trial of cognitive-behavioral therapy for augmenting pharmacotherapy in obsessive-compulsive disorder
Abstract
Objective: Although serotonin reuptake inhibitors (SRIs) are approved for the treatment of obsessive-compulsive disorder (OCD), most OCD patients who have received an adequate SRI trial continue to have clinically significant OCD symptoms. The purpose of this study was to examine the effects of augmenting SRIs with exposure and ritual prevention, an established cognitive-behavioral therapy (CBT) for OCD.
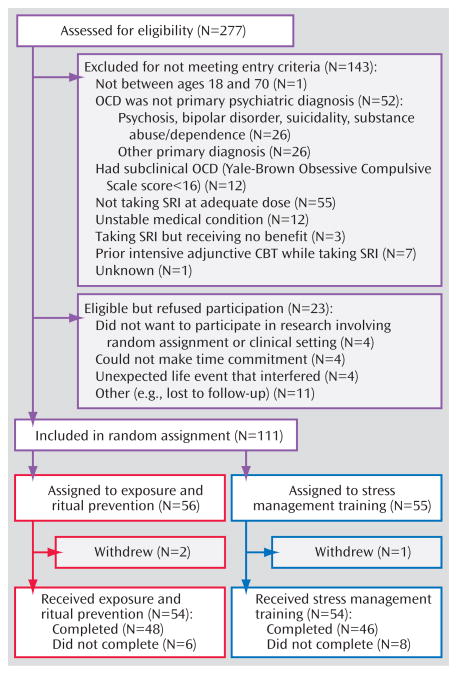
Method: A randomized, controlled trial was conducted at two academic outpatient clinics to compare the effects of augmenting SRIs with exposure and ritual prevention versus stress management training, another form of CBT. Participants were adult outpatients (N=108) with primary OCD and a Yale-Brown Obsessive Compulsive Scale total score > or = 16 despite a therapeutic SRI dose for at least 12 weeks prior to entry. Participants received 17 sessions of CBT (either exposure and ritual prevention or stress management training) twice a week while continuing SRI pharmacotherapy.
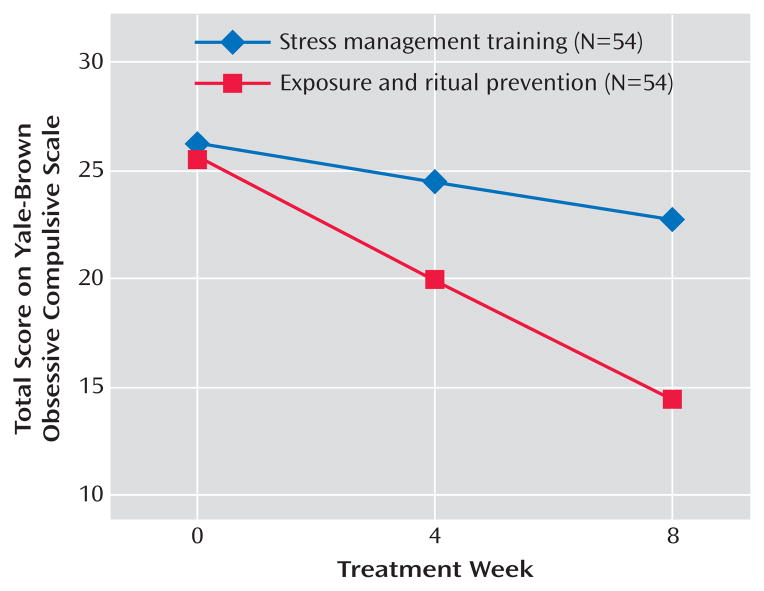
Results: Exposure and ritual prevention was superior to stress management training in reducing OCD symptoms. At week 8, significantly more patients receiving exposure and ritual prevention than patients receiving stress management training had a decrease in symptom severity of at least 25% (based on Yale-Brown Obsessive Compulsive Scale scores) and achieved minimal symptoms (defined as a Yale-Brown Obsessive Compulsive Scale score < or = 12).
Conclusions: Augmentation of SRI pharmacotherapy with exposure and ritual prevention is an effective strategy for reducing OCD symptoms. However, 17 sessions were not sufficient to help most of these patients achieve minimal symptoms.
Conflict of interest statement
All remaining authors report no competing interests.
Figures
Comment in
-
Exposure and ritual prevention reduces symptoms more than stress management training in OCD treated with SSRIs.Evid Based Ment Health. 2009 Feb;12(1):17. doi: 10.1136/ebmh.12.1.17. Evid Based Ment Health. 2009. PMID: 19176776 No abstract available.
References
-
- American Psychiatric Association. Practice guideline for the treatment of patients with obsessive-compulsive disorder. Am J Psychiatry. 2007;164(suppl):1–56. - PubMed
-
- Blanco C, Olfson M, Stein DJ, Simpson HB, Gameroff MJ, Narrow WH. Treatment of obsessive-compulsive disorder by U.S. psychiatrists. J Clin Psychiatry. 2006;67:946–951. - PubMed
-
- Pigott TA, Seay SM. A review of the efficacy of selective serotonin reuptake inhibitors in obsessive-compulsive disorder. J Clin Psychiatry. 1999;60:101–106. - PubMed
-
- Bloch MH, Landeros-Weisenberger A, Kelmendi B, Coric V, Bracken MB, Leckman JF. A systematic review: antipsychotic augmentation with treatment refractory obsessive-compulsive disorder. Mol Psychiatry. 2006;11:622–632. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
