

Pathogenesis of ovarian cancer: lessons from morphology and molecular biology and their clinical implications
- PMID: 18317228
- PMCID: PMC2794425
- DOI: 10.1097/PGP.0b013e318161e4f5
Pathogenesis of ovarian cancer: lessons from morphology and molecular biology and their clinical implications
Abstract
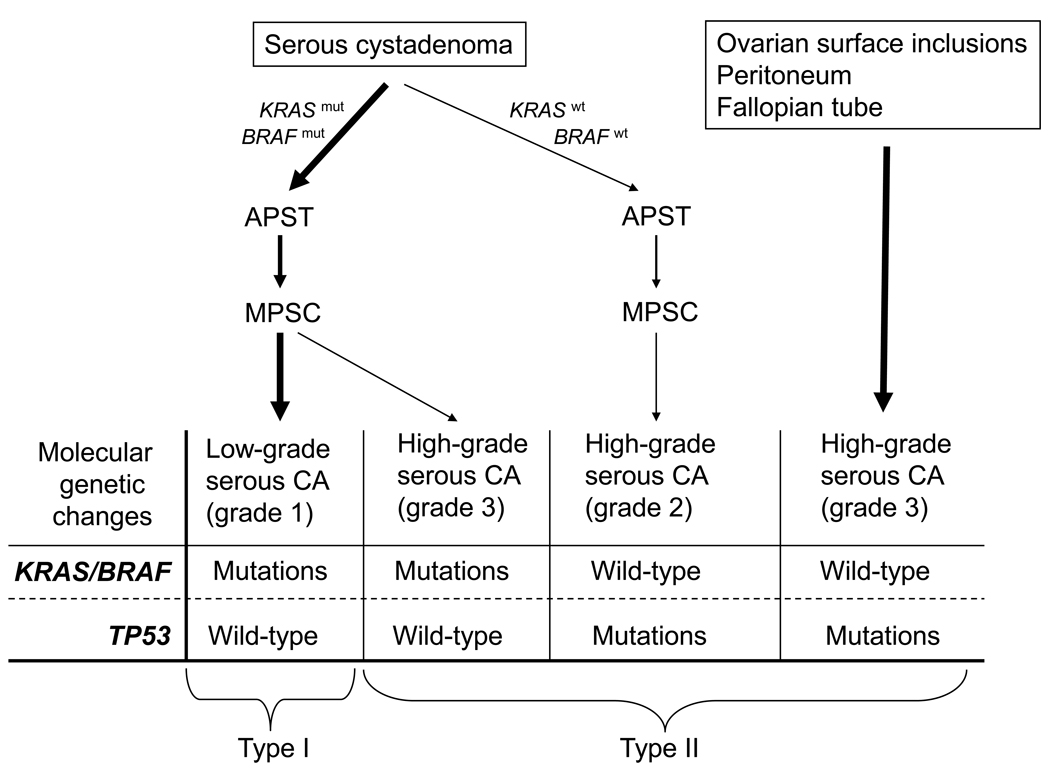
The accepted view of ovarian carcinogenesis is that carcinoma begins in the ovary, undergoes progressive "dedifferentiation" from a well to a poorly differentiated tumor, and then spreads to the pelvic and abdominal cavities before metastasizing to distant sites. It has therefore been reasoned that survival for this highly lethal disease could be improved by developing screening methods that detect disease when it is confined to the ovary. To date, however, no prospective randomized trial of any ovarian cancer screening test(s) has demonstrated a decrease in mortality. We believe that one of the main reasons for this is that the dogma underlying ovarian carcinogenesis is flawed. Based on studies performed in our laboratory during the last decade, we have proposed a model of ovarian carcinogenesis that takes into account the diverse nature of ovarian cancer and correlates the clinical, pathological, and molecular features of the disease. In this model, ovarian tumors are divided into 2 groups designated type I and type II. Type I tumors are slow growing, generally confined to the ovary at diagnosis, and develop from well-established precursor lesions that are termed "borderline" tumors. Type I tumors include low-grade micropapillary serous carcinoma, mucinous, endometrioid, and clear cell carcinomas. They are genetically stable and are characterized by mutations in a number of different genes including KRAS, BRAF, PTEN, and beta-catenin. Type II tumors are rapidly growing highly aggressive neoplasms for which well-defined precursor lesions have not been described. Type II tumors include high-grade serous carcinoma, malignant mixed mesodermal tumors (carcinosarcomas), and undifferentiated carcinomas. This group of tumors has a high level of genetic instability and is characterized by mutation of TP53. The model helps to explain why current screening techniques, aimed at detecting stage I disease, have not been effective. Tumors that remain confined to the ovary for a long period belong to the type I group, but they account for only 25% of the malignant tumors. Most of what is considered ovarian cancer belongs to the type II category, and these are only rarely confined to the ovary. Although the reasons for this are not entirely clear, possible explanations include rapid spread from the ovary early in carcinogenesis and development of carcinoma in extra ovarian sites, notably, the peritoneum and fallopian tube, with secondary involvement of the ovary. The latter tumors are advanced stage at their inception. Therefore, a more realistic end point for the early detection of ovarian cancer is volume and not stage of disease. The model does not replace the histopathologic classification but, by drawing attention to the molecular genetic events that play a role in tumor progression, sheds light on new approaches to early detection and treatment.
Figures
References
-
- Burks RT, Sherman ME, Kurman RJ. Micropapillary serous carcinoma of the ovary. A distinctive low-grade carcinoma related to serous borderline tumors. Am J Surg Pathol. 1996;20:1319–1330. - PubMed
-
- Seidman JD, Russell P, Kurman RJ. Surface epithelial tumors of the ovary. In: Kurman RJ, editor. Blaustein's Pathology of the Female Genital Tract. 5th ed. New York: Springer Verlag; 2002. pp. 791–904.
-
- Seidman JD, Kurman RJ. Subclassification of serous borderline tumors of the ovary into benign and malignant types. A clinicopathologic study of 65 advanced stage cases. Am J Surg Pathol. 1996;20:1331–1345. - PubMed
-
- Shih Ie M, Kurman RJ. Molecular pathogenesis of ovarian borderline tumors: new insights and old challenges. Clin Cancer Res. 2005;11:7273–7279. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
