

Why don't diabetes patients achieve recommended risk factor targets? Poor adherence versus lack of treatment intensification
- PMID: 18317847
- PMCID: PMC2324158
- DOI: 10.1007/s11606-008-0554-8
Why don't diabetes patients achieve recommended risk factor targets? Poor adherence versus lack of treatment intensification
Abstract
Background: Despite the availability of effective hypertension, hyperlipidemia, and hyperglycemia therapies, target levels of systolic blood pressure (SBP), LDL-cholesterol (LDL-c), and hemoglobin A1c control are often not achieved.
Objective: To examine the relative importance of patient medication nonadherence versus clinician lack of therapy intensification in explaining above target cardiovascular disease (CVD) risk factor levels.
Design: Cross-sectional assessment.
Participants: In 2005, 161,697 Kaiser Permanente Northern California adult diabetes patients were included in the study.
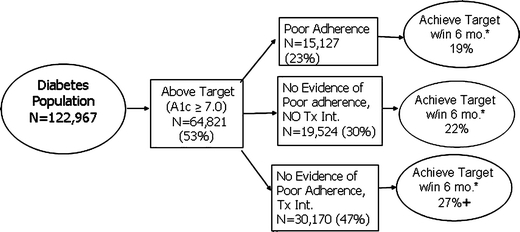
Measurement: "Above target" was defined as most recent A1c >/=7.0% for hyperglycemia, LDL-c >/=100 mg/dL for hyperlipidemia, and SBP >/=130 mmHg for hypertension. Poor adherence was defined as medication gaps for >/=20% of days covered for all medications for each condition separately. Treatment intensification was defined as an increase in the number of drug classes, increased dosage of a class, or a switch to a different class within the 3 months before or after notation of above target levels.
Results: Poor adherence was found in 20-23% of patients across the 3 conditions. No evidence of poor adherence with no treatment intensification was found in 30% of hyperglycemia patients, 47% of hyperlipidemia patients, and 36% of hypertension patients. Poor adherence or lack of therapy intensification was evident in 53-68% of patients above target levels across conditions.
Conclusions: Both nonadherence and lack of treatment intensification occur frequently in patients above target for CVD risk factor levels; however, lack of therapy intensification was somewhat more common. Quality improvement efforts should focus on these modifiable barriers to CVD risk factor control.
Figures


Comment in
-
Poor outcomes in diabetes care: is medication nonadherence or lack of treatment intensification to blame?Nat Clin Pract Endocrinol Metab. 2008 Oct;4(10):536-7. doi: 10.1038/ncpendmet0926. Epub 2008 Aug 5. Nat Clin Pract Endocrinol Metab. 2008. PMID: 18679385 No abstract available.
References
-
- Neyer JR, Greenlund KJ, Denny CH, Keenan NL, Labarthe DR, Croft JB. Prevalence of heart disease—United States, 2005. JAMA. 2007;297:1308–9. - DOI
-
- Pearson TA, Blair SN, Daniels S, et al. AHA guidelines for primary prevention of cardiovascular disease and stroke: 2002 update: consensus panel guide to comprehensive risk reduction for adult patients without coronary or other atherosclerotic vascular diseases. American Heart Association Science Advisory and Coordinating Committee. Circulation. 2002;106:388–91. - DOI - PubMed
-
- Anonymous. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet. 1994;344:1383–9. - PubMed
