

Ability of pleth variability index to detect hemodynamic changes induced by passive leg raising in spontaneously breathing volunteers
- PMID: 18325089
- PMCID: PMC2447559
- DOI: 10.1186/cc6822
Ability of pleth variability index to detect hemodynamic changes induced by passive leg raising in spontaneously breathing volunteers
Abstract
Introduction: Pleth Variability Index (PVI) is a new algorithm that allows continuous and automatic estimation of respiratory variations in the pulse oximeter waveform amplitude. Our aim was to test its ability to detect changes in preload induced by passive leg raising (PLR) in spontaneously breathing volunteers.
Methods: We conducted a prospective observational study. Twenty-five spontaneously breathing volunteers were enrolled. PVI, heart rate and noninvasive arterial pressure were recorded. Cardiac output was assessed using transthoracic echocardiography. Volunteers were studied in three successive positions: baseline (semirecumbent position); after PLR of 45 degrees with the trunk lowered in the supine position; and back in the semirecubent position.
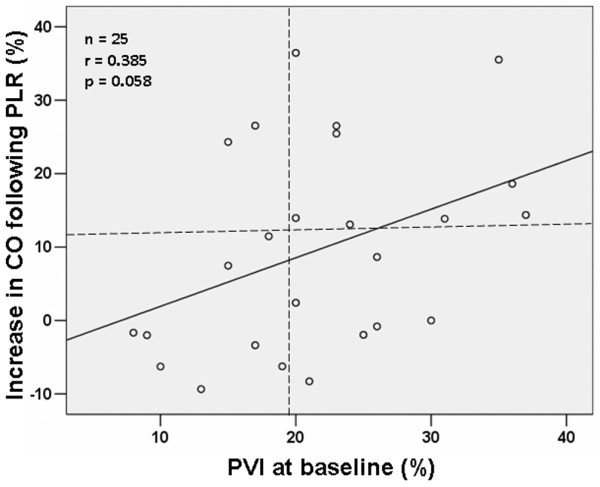
Results: We observed significant changes in cardiac output and PVI during changes in body position. In particular, PVI decreased significantly from baseline to PLR (from 21.5 +/- 8.0% to 18.3 +/- 9.4%; P < 0.05) and increased significantly from PLR to the semirecumbent position (from 18.3 +/- 9.4% to 25.4 +/- 10.6 %; P < 0.05). A threshold PVI value above 19% was a weak but significant predictor of response to PLR (sensitivity 82%, specificity 57%, area under the receiver operating characteristic curve 0.734 +/- 0.101).
Conclusion: PVI can detect haemodynamic changes induced by PLR in spontaneously breathing volunteers. However, we found that PVI was a weak predictor of fluid responsiveness in this setting.
Figures




References
-
- Cannesson M, Attof Y, Rosamel P, Desebbe O, Joseph P, Metton O, Bastien O, Lehot JJ. Respiratory variations in pulse oximetry plethysmographic waveform amplitude to predict fluid responsiveness in the operating room. Anesthesiology. 2007;106:1105–1111. doi: 10.1097/01.anes.0000267593.72744.20. - DOI - PubMed
-
- Michard F, Boussat S, Chemla D, Anguel N, Mercat A, Lecarpentier Y, Richard C, Pinsky MR, Teboul JL. Relation between respiratory changes in arterial pulse pressure and fluid responsiveness in septic patients with acute circulatory failure. Am J Respir Crit Care Med. 2000;162:134–138. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
