

Approach to the adult with congenital adrenal hyperplasia due to 21-hydroxylase deficiency
- PMID: 18326005
- PMCID: PMC2266964
- DOI: 10.1210/jc.2007-2417
Approach to the adult with congenital adrenal hyperplasia due to 21-hydroxylase deficiency
Abstract
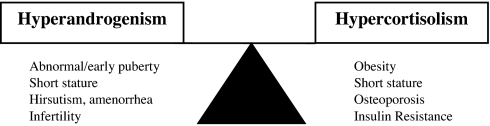
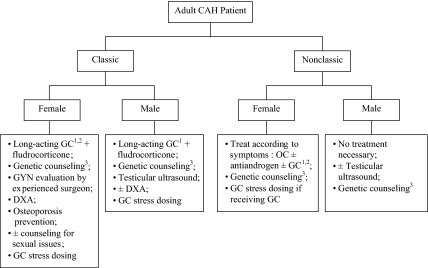
Congenital adrenal hyperplasia (CAH) describes a group of autosomal recessive disorders where there is impairment of cortisol biosynthesis. CAH due to 21-hydroxylase deficiency accounts for 95% of cases and shows a wide range of clinical severity. Treatment of the classic or severe form of CAH is targeted at replacing cortisol and aldosterone and effectively controlling excess androgen symptoms by using the lowest possible glucocorticoid dose. Treatment of the mild or nonclassic form is targeted at controlling excess androgen symptoms and may or may not involve glucocorticoid therapy. Hydrocortisone is the treatment of choice for children, but there is no consensus on how patients should be treated as adults. Current glucocorticoid therapy is suboptimal because it is often difficult to reduce excess androgen without giving excess glucocorticoid, and patients may experience hypercortisolism, androgen excess, or a combination of these states. Treatment of CAH, especially in the adult patient, remains controversial given the lack of prospective randomized controlled trials comparing treatment regimens. Nevertheless, patients benefit from careful individualized therapy with avoidance of Cushingoid side effects and optimization of reproductive, sexual, and bone health.
Figures
References
-
- Merke DP, Bornstein SR 2005 Congenital adrenal hyperplasia. Lancet 365:2125–2136 - PubMed
-
- Jaaskelainen J, Levo A, Voutilainen R, Partanen J 1997 Population-wide evaluation of disease manifestation in relation to molecular genotype in steroid 21-hydroxylase (CYP21) deficiency: good correlation in a well defined population. J Clin Endocrinol Metab 82:3293–3297 - PubMed
-
- Krone N, Braun A, Roscher AA, Knorr D, Schwarz HP 2000 Predicting phenotype in steroid 21-hydroxylase deficiency? Comprehensive genotyping in 155 unrelated, well defined patients from southern Germany. J Clin Endocrinol Metab 85:1059–1065 - PubMed
-
- Wedell A, Thilen A, Ritzen EM, Stengler B, Luthman H 1994 Mutational spectrum of the steroid 21-hydroxylase gene in Sweden: implications for genetic diagnosis and association with disease manifestation. J Clin Endocrinol Metab 78:1145–1152 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
