

Quantifying tibial plafond fracture severity: absorbed energy and fragment displacement agree with clinical rank ordering
- PMID: 18327811
- PMCID: PMC2562904
- DOI: 10.1002/jor.20550
Quantifying tibial plafond fracture severity: absorbed energy and fragment displacement agree with clinical rank ordering
Abstract
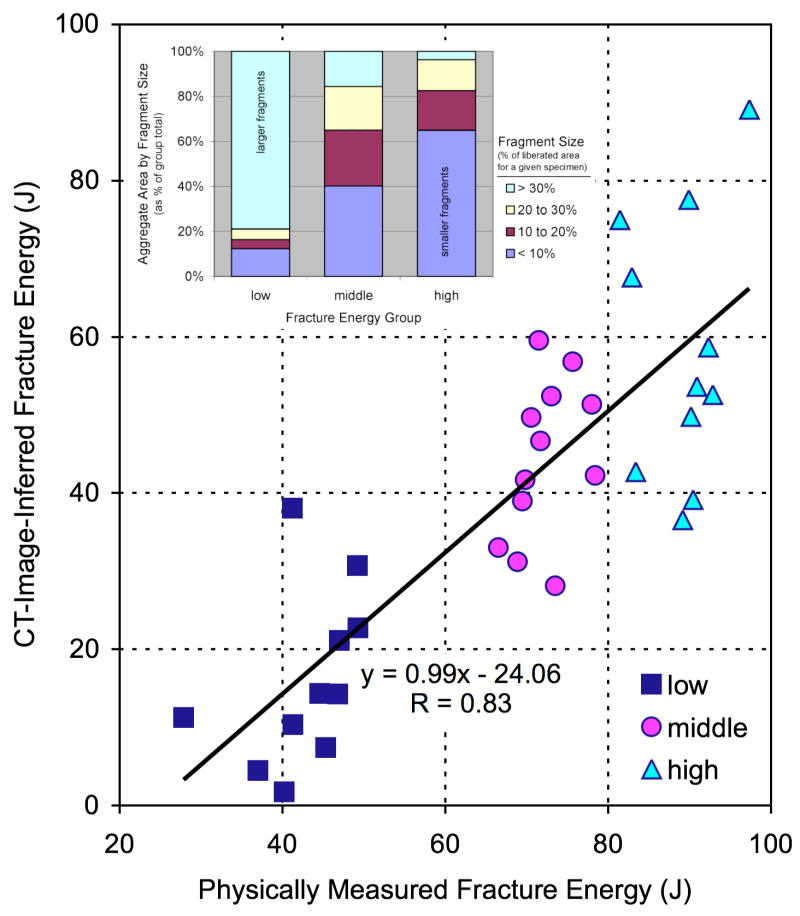
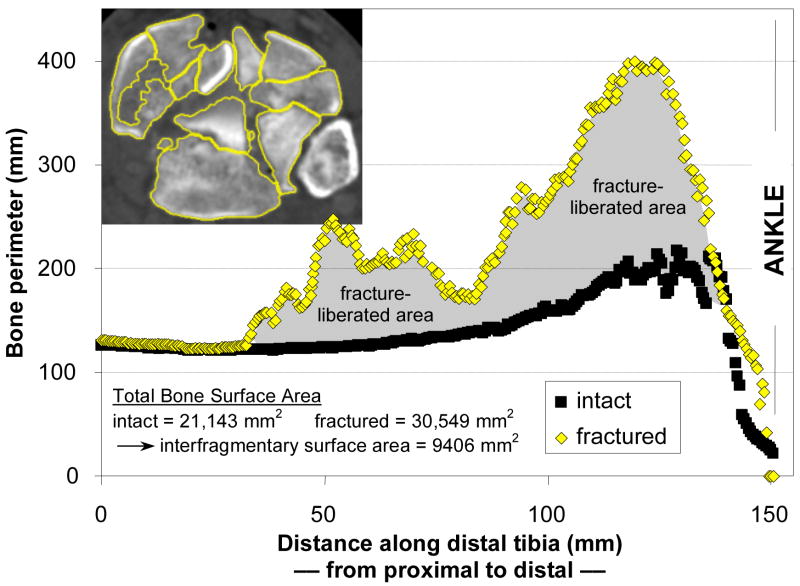
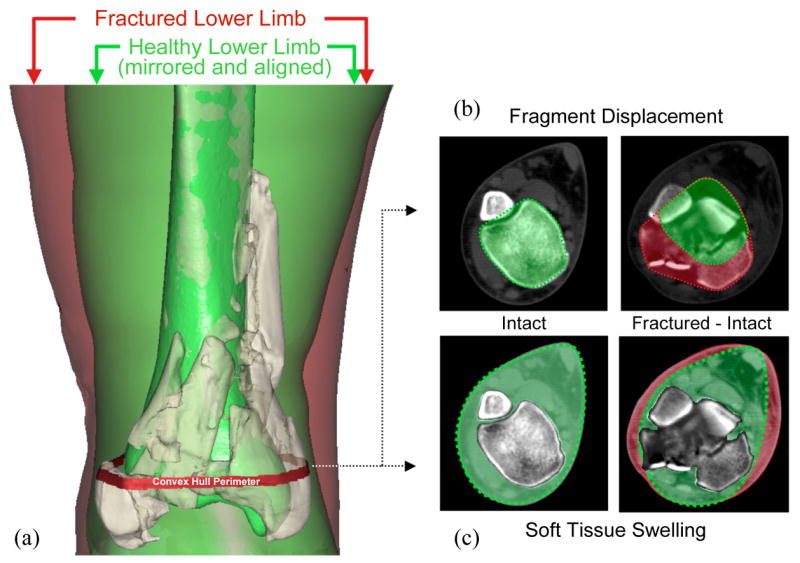
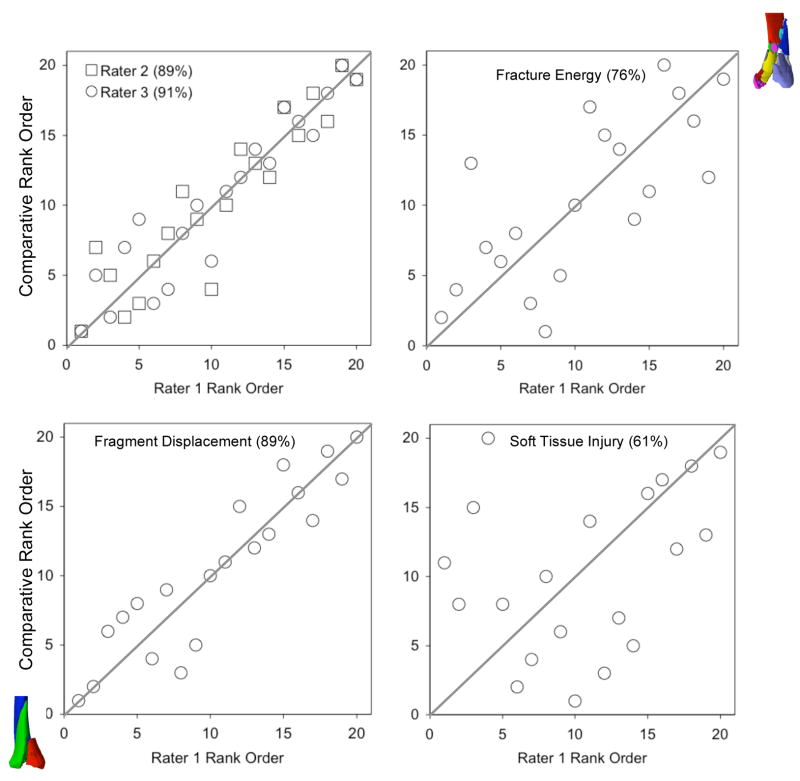
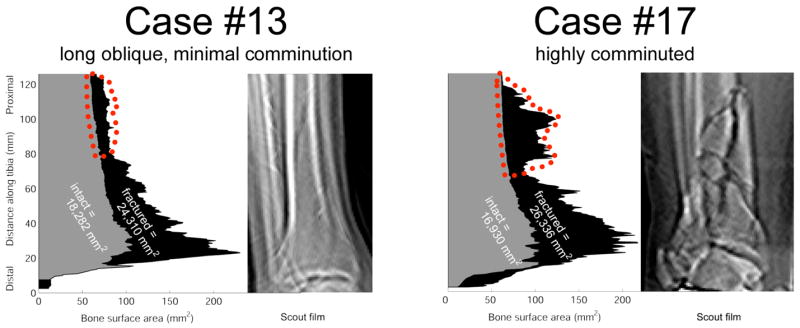
The energy of producing a fracture is considered one of the most important factors relating to injury severity, prognosis, and risk of complications, yet there has been no objective way to measure this important variable. The purpose of this study was to compare assessments of fracture severity made using new objective computed tomography (CT)-based methods versus the expert opinion of experienced orthopedic traumatologists. Fracture energy, fragment displacement, and soft tissue swelling were quantified in twenty tibial plafond fractures by analyzing injury CT scans. Three experienced orthopedic traumatologists then independently performed a rank order analysis of fracture severity, using plain radiographs. The concordance among the three clinicians ranged from 87% to 91%. Objective fracture severity measurements made with the CT algorithm agreed well with the clinical assessments (fracture energy concordance from 73% to 76%, fragment displacement from 82% to 89%, and soft tissue swelling from 61% to 65%). These are the first objective, CT-based measures of fracture severity. With further refinement, this conceptually novel method has the potential to serve as a valuable tool to provide objective measurement of fracture severity, allowing one to control for this previously confounding variable in large multicenter studies.
Figures

References
-
- Wyrsch B, McFerran MA, McAndrew M, et al. Operative treatment of fractures of the tibial plafond. J Bone Joint Surg Am. 1996;78:1646–1657. - PubMed
-
- Crutchfield E, Seligson D, Henry S, Warnholtz A. Tibial pilon fractures: a comparative clinical study of management techniques and results. Orthopedics. 1995;18:613–617. - PubMed
-
- Evangelopoulos D, Anastasakis D, Samelis P, Vlachopoulos J. Articular fractures of the tibia (pilon) grade III. Treatment with external fixator and minimal internal fixation. J Bone Joint Surg Br. 1999;81(Suppl II):181.
-
- Hernandez JA, Rodriguez D, Garreta JL, et al. Fractures of the tibial plafond. Influence of fracture type and accuracy of articular reduction in their prognosis. J Bone Joint Surg Br. 1999;81(Suppl II):181.
-
- Stojkovska E, Saveski J, Todorov I, et al. Results of surgical treatment of displaced pilon fractures. J Bone Joint Surg Br. 1999;81(Suppl II):181.
