

Unilateral subthalamic nucleus stimulation has a measurable ipsilateral effect on rigidity and bradykinesia in Parkinson disease
- PMID: 18329019
- PMCID: PMC2413293
- DOI: 10.1016/j.expneurol.2008.01.024
Unilateral subthalamic nucleus stimulation has a measurable ipsilateral effect on rigidity and bradykinesia in Parkinson disease
Abstract
Background: Bilateral deep brain stimulation (DBS) of the subthalamic nucleus (STN) improves motor function in Parkinson disease (PD). However, little is known about the quantitative effects on motor behavior of unilateral STN DBS.
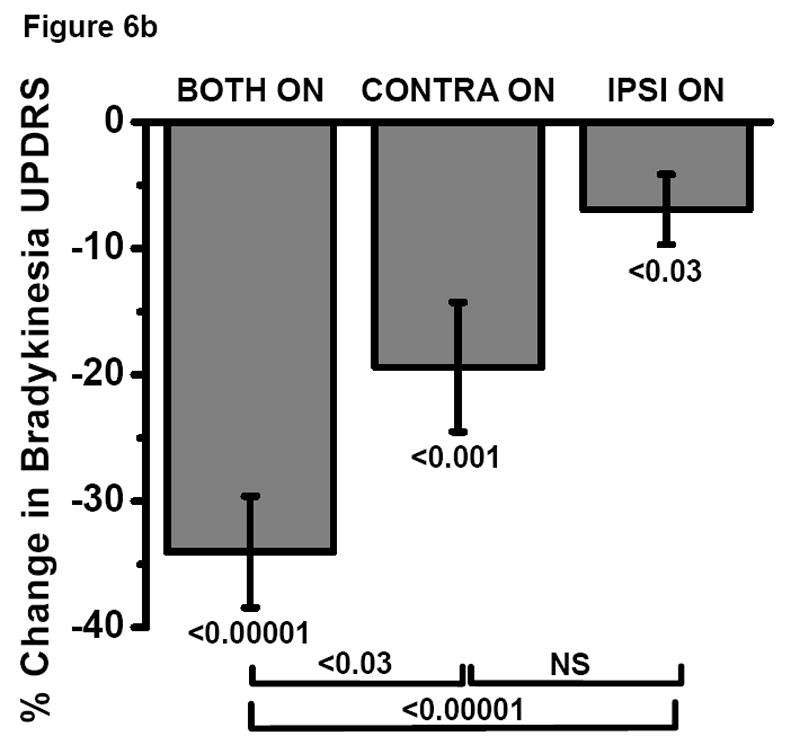
Methods: In 52 PD subjects with STN DBS, we quantified in a double-blinded manner rigidity (n=42), bradykinesia (n=38), and gait speed (n=45). Subjects were tested in four DBS conditions: both on, left on, right on and both off. A force transducer was used to measure rigidity across the elbow, and gyroscopes were used to measure angular velocity of hand rotations for bradykinesia. About half of the subjects were rated using the Unified Parkinson Disease Rating Scale (part III) motor scores for arm rigidity and repetitive hand rotation simultaneously during the kinematic measurements. Subjects were timed walking 25 feet.
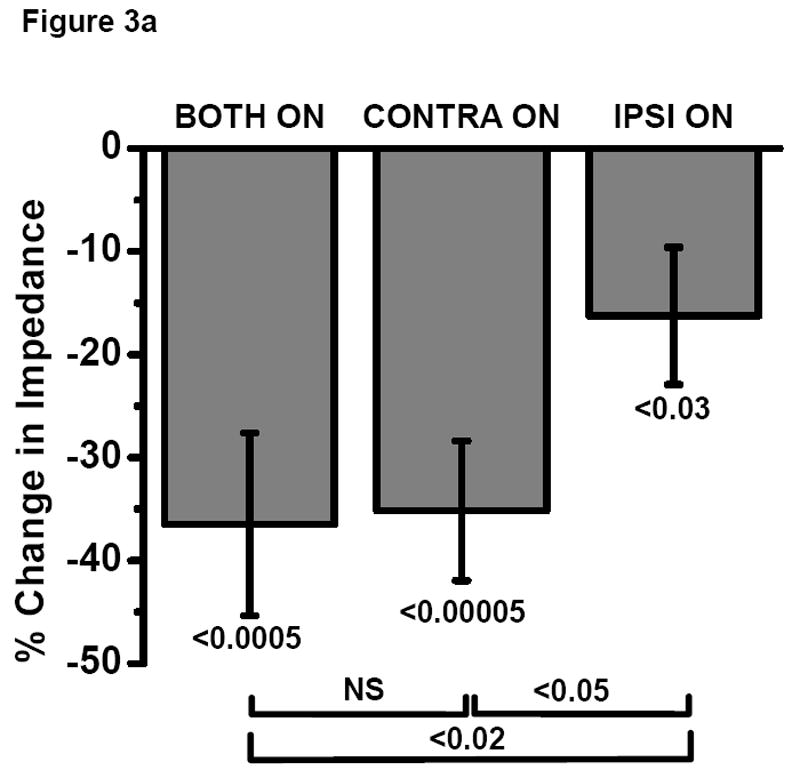
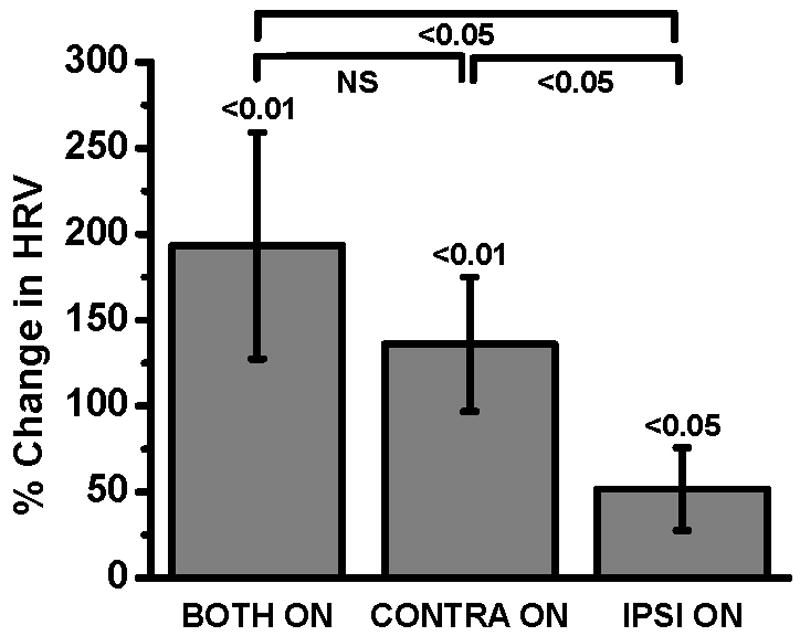
Results: All subjects had significant improvement with bilateral STN DBS. Contralateral, ipsilateral and bilateral stimulation significantly reduced rigidity and bradykinesia. Bilateral stimulation improved rigidity more than unilateral stimulation of either side, but there was no significant difference between ipsilateral and contralateral stimulation. Although bilateral stimulation also increased hand rotation velocity more than unilateral stimulation of either side, contralateral stimulation increased hand rotation significantly more than ipsilateral stimulation. All stimulation conditions improved walking time but bilateral stimulation provided the greatest improvement.
Conclusions: Unilateral STN DBS decreased rigidity and bradykinesia contralaterally as well ipsilaterally. As expected, bilateral DBS improved gait more than unilateral DBS.
Figures






References
-
- Allert N, Volkmann J, Dotse S, Hefter H, Sturm V, Freund HJ. Effects of bilateral pallidal or subthalamic stimulation on gait in advanced Parkinson's disease. Mov Disord. 2001;16:1076–1085. - PubMed
-
- Bastian AJ, Kelly VE, Revilla FJ, Perlmutter JS, Mink JW. Different effects of unilateral versus bilateral subthalamic nucleus stimulation on walking and reaching in Parkinson's disease. Mov Disord. 2003;18:1000–1007. - PubMed
-
- Burchiel KJ, Anderson VC, Favre J, Hammerstad JP. Comparison of pallidal and subthalamic nucleus deep brain stimulation for advanced Parkinson's disease: results of a randomized, blinded pilot. Neurosurgery. 1999;45:1375–1382. - PubMed
-
- Calne DB, Snow BJ, Lee C. Criteria for diagnosing Parkinson's disease. Ann Neurol. 1992;32:S125–S127. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
