

Scleroderma-like fibrosing disorders
- PMID: 18329541
- PMCID: PMC2706095
- DOI: 10.1016/j.rdc.2007.11.001
Scleroderma-like fibrosing disorders
Abstract
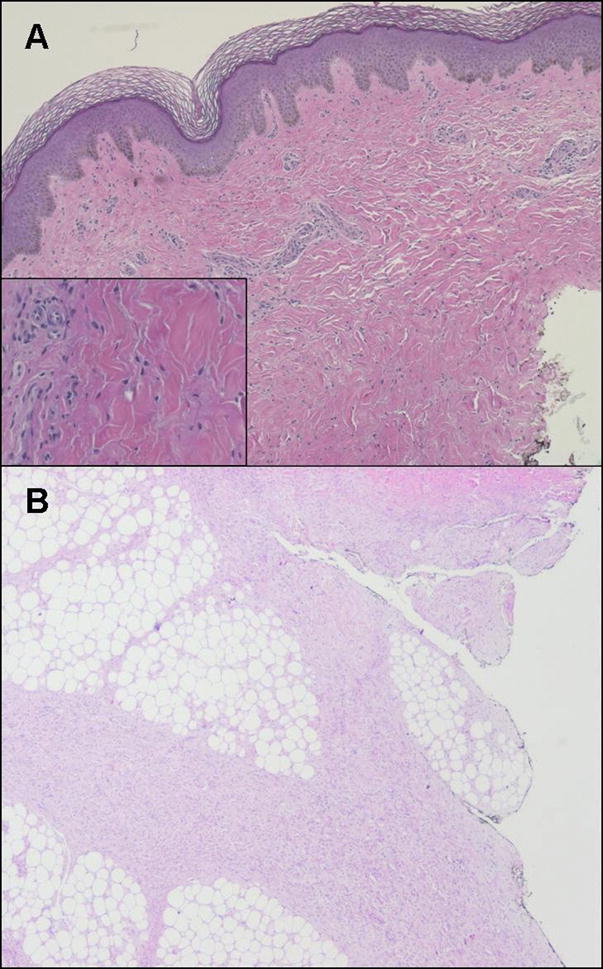
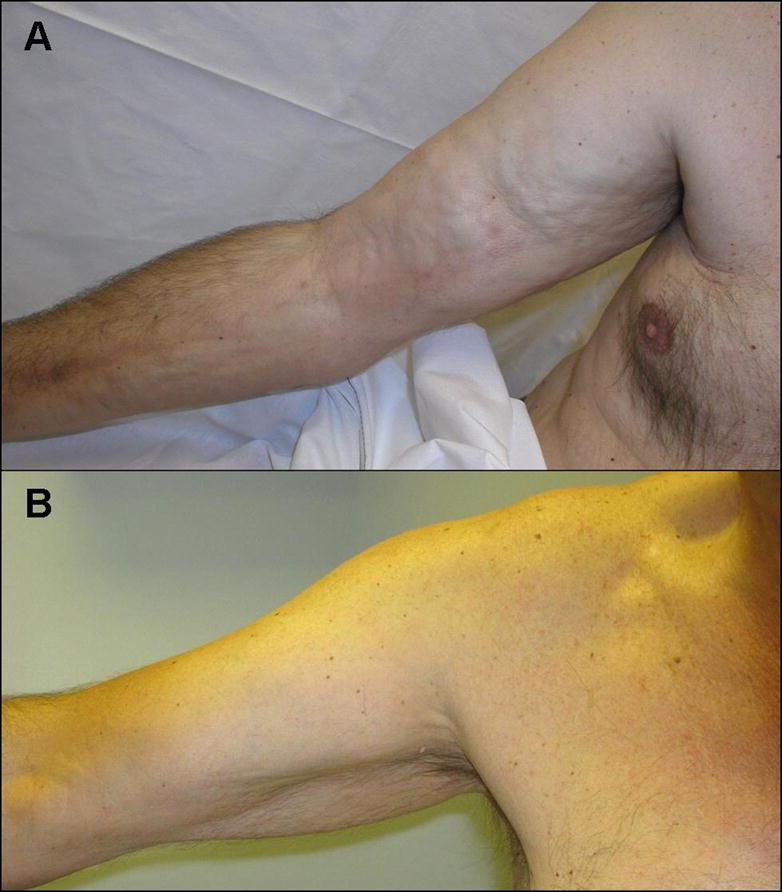
Many conditions presenting with clinical hard skin and tissue fibrosis can be confused with systemic sclerosis (scleroderma). These disorders have very diverse etiologies and often an unclear pathogenetic mechanism. Distinct clinical characteristics, skin histology, and disease associations may allow one to distinguish these conditions from scleroderma and from each other. A prompt diagnosis is important to spare patients from ineffective treatments and inadequate management. This article highlights nephrogenic systemic fibrosis (nephrogenic fibrosing dermopathy), eosinophilic fasciitis (Shulman's syndrome), scleromyxedema, and scleredema. These often are detected in the primary care setting and referred to rheumatologists for further evaluation. Rheumatologists must be able to promptly recognize them to provide valuable prognostic information and appropriate treatment options for affected patients.
Figures


References
-
- Cowper SE, Robin HS, Steinberg SM, et al. Scleromyxoedema-like cutaneous diseases in renal-dialysis patients. Lancet. 2000;356(9234):1000–1. - PubMed
-
- Jan F, Segal JM, Dyer J, et al. Nephrogenic fibrosing dermopathy: two pediatric cases. J Pediatr. 2003;143(5):678–81. - PubMed
-
- Cowper SE. Nephrogenic Fibrosing Dermopathy NFD/NSF Website. 2001–2007. [Accessed 11/05/2007]. Available at http://www.icnfdr.org. - PubMed
-
- Cowper SE, Su LD, Bhawan J, et al. Nephrogenic fibrosing dermopathy. Am J Dermatopathol. 2001;23(5):383–93. - PubMed
-
- Ting WW, Stone MS, Madison KC, et al. Nephrogenic fibrosing dermopathy with systemic involvement. Arch Dermatol. 2003;139(7):903–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
