

Microanatomy and surgical approaches to the infratemporal fossa: an anaglyphic three-dimensional stereoscopic printing study
- PMID: 18330427
- PMCID: PMC2095118
- DOI: 10.1055/s-2007-985193
Microanatomy and surgical approaches to the infratemporal fossa: an anaglyphic three-dimensional stereoscopic printing study
Abstract
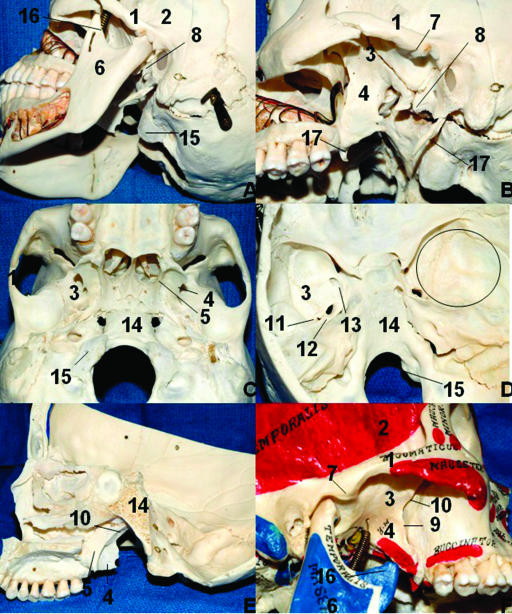
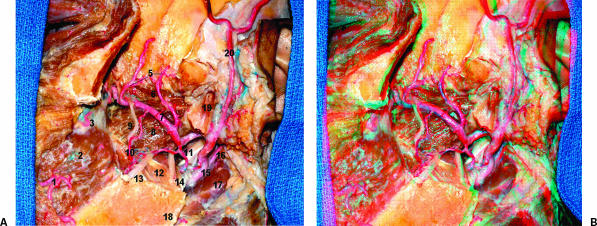
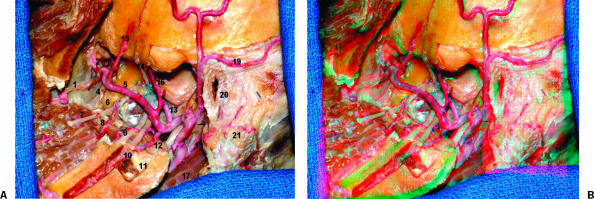
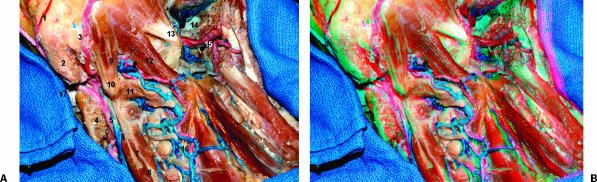
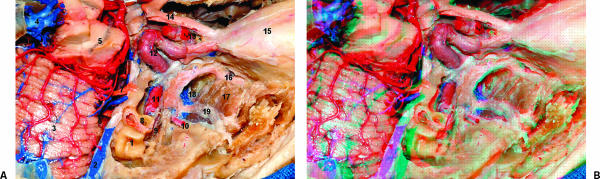
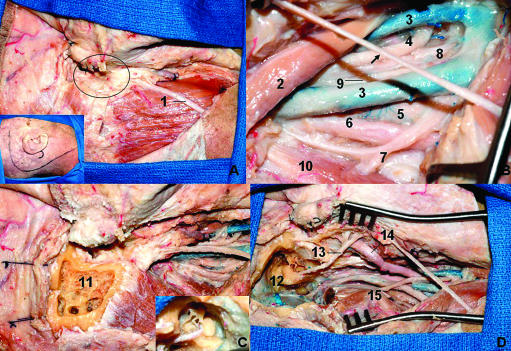
Objective: The infratemporal fossa (ITF) is a continuation of the temporal fossa between the internal surface of the zygoma and the external surface of the temporal bone and greater wing of the sphenoid bone that is sitting deep to the ramus of the mandible. The principal structure to understanding its relationships is the lateral pterygoid muscle. Other important structures are the medial pterygoid muscle, the maxillary artery, the pterygoid venous plexus, the otic ganglion, the chorda tympani nerve and the mandibular nerve. In this study, we describe the microsurgical anatomy of the ITF, as viewed by step-by-step anatomical dissection and also through the perspective of three lateral approaches and one anterior surgical approach.
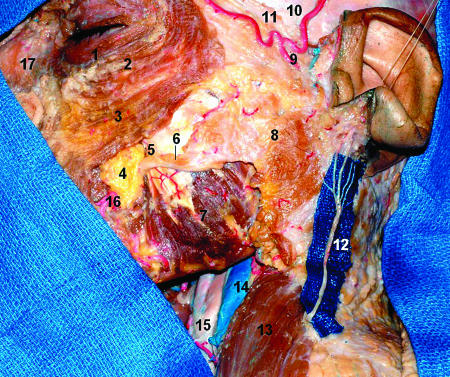
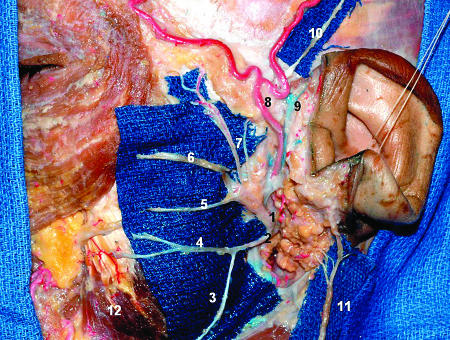
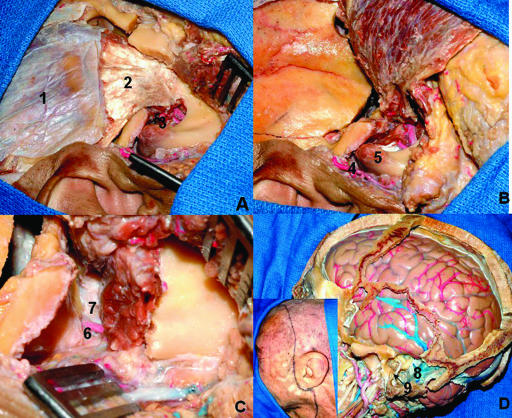
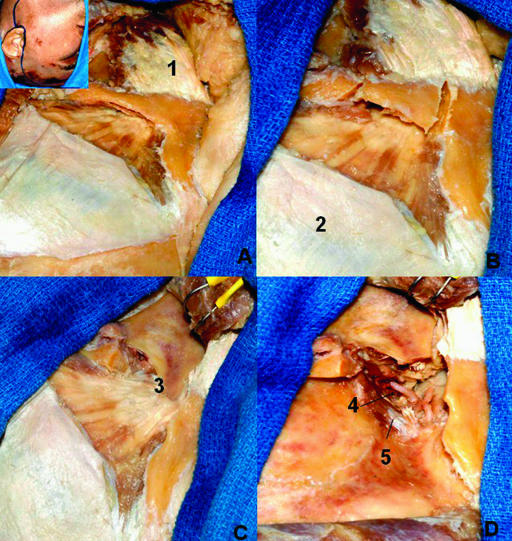
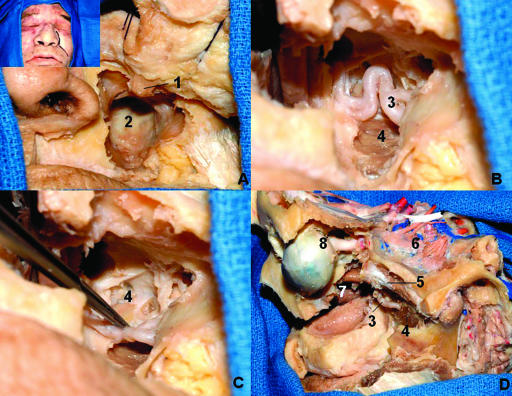
Methods: Eight cadaver specimens were dissected. In one side of all specimens, an anatomical dissection was done in which a wide preauricular incision from the neck on the anterior border of the sternoclidomastoid muscle at the level of the cricoid cartilage to the superior temporal line was made. The flap was displaced anteriorly and the structures of the neck were dissected followed by a zygomatic osteotomy and dissection of the ITF structures. On the other side were the surgical approaches to the ITF. The combined infratemporal and posterior fossa approach was done in two specimens, the subtemporal preauricular infratemporal fossa approach in two, the zygomatic approach in two, and the lateral transantral maxillotomy in two. The anatomical dissections were documented on the three-dimensional (3D) anaglyphic method to produce stereoscopic prints.
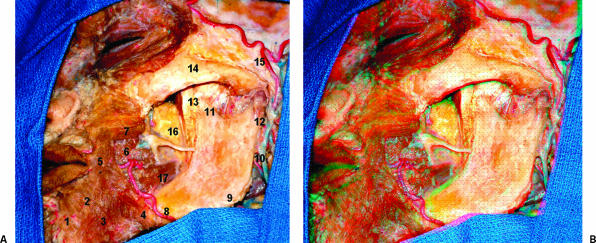
Results: The lateral pterygoid muscle is one of the principal structures to enable understanding of the relationships into the ITF. The tendon of the temporal muscle inserts in the coronoid process at the ITF. The maxillary artery is the terminal branch of the external carotid artery that originates at the neck of the mandible and runs into the parotid gland. In our dissections the maxillary artery was lateral to the buccal, lingual, and inferior alveolar nerves. We found the second part of the maxillary artery superficial to the lateral pterygoid muscle in all specimens The anterior and posterior branches of the deep temporal artery supply the temporal muscle. In two cases we found a middle deep temporal artery. The different approaches that we used provided different views of the same anatomical landmarks and this provides not only safer surgery but also the best choice to approach the ITF according with the pathology extension.
Conclusions: The ITF is a complex region on the skull base that is affected by benign and malignant tumors. The study through different routes is helpful to disclose the relationship among the anatomical structures. Although the authors have shown four approaches, there are a variety of approaches and even a combination of these can be used. This type of anatomical knowledge is essential to choosing the best approach to treat lesions in this area.
Keywords: Infratemporal fossa; approaches; mandibular nerve; paraganglioma; surgical anatomy.
Figures

References
-
- Gray H. Anatomy of the Human Body. New York: Bartley.com; 2000.
-
- Vrionis F D, Cano W G, Heilman C B. Microsurgical anatomy of the infratemporal fossa as viewed laterally and superiorly. Neurosurgery. 1996;39:777–786. - PubMed
-
- Bejjani G K, Sullivan B, Salas-Lopez E, et al. Surgical anatomy of the infratemporal fossa: the styloid diaphragm revisited. Neurosurgery. 1998;43:842–852. - PubMed
-
- Schramm V L., Jr In: Sekhar LN, Schramm VL, editor. Tumors of the Cranial Base: Diagnosis and Treatment. Mount Kisco, NY: Futura Publishing Co; 1987. Infratemporal fossa surgery. pp. 421–437.
-
- Ribas G C, Bento R F, Rodrigues A J. Anaglyphic three-dimensional stereoscopic printing: revival of an old method for anatomical and surgical teaching and reporting. J Neurosurg. 2001;95:1057–1066. - PubMed
