

Endovascular treatment of tiny ruptured anterior communicating artery aneurysms
- PMID: 18330519
- PMCID: PMC2440929
- DOI: 10.1007/s00234-008-0371-0
Endovascular treatment of tiny ruptured anterior communicating artery aneurysms
Abstract
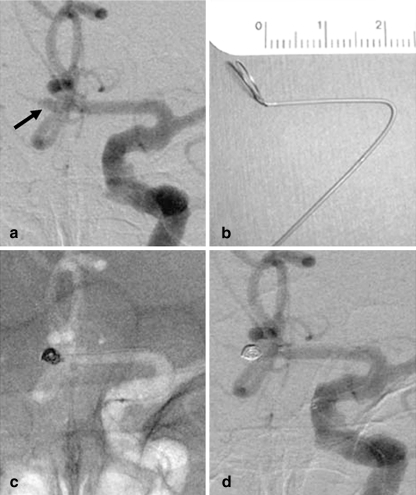
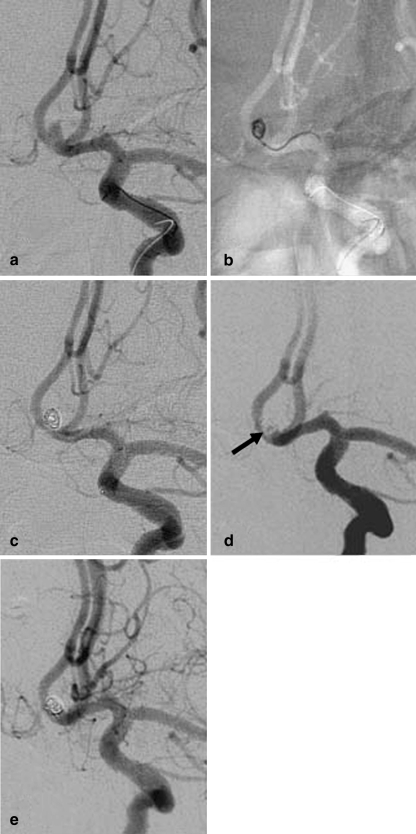
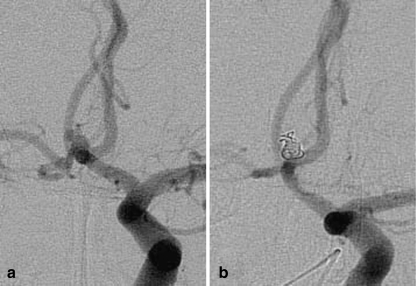
Introduction: Because of its high complication rate, the endovascular treatment (EVT) of anterior communicating artery (ACoA) aneurysms less than 3 mm in maximum diameter remains controversial. We evaluated EVT of tiny ruptured ACoA aneurysms with Guglielmi detachable coils (GDCs).
Methods: We treated 19 ruptured ACoA aneurysms with a maximum diameter of <or=3 mm with GDCs. The pretreatment Hunt and Hess score was grade 1 in four patients, grade 2 in six, grade 3 in six, and grade 4 in three. The patients were clinically assessed before and after treatment and with multiple angiographic follow-up studies.
Results: All EVTs were successful; there were no aneurysm perforations or any other treatment-related complications. In five patients older than 80 years the transfemoral approach was difficult, and the direct carotid approach was used. Complete and near-complete occlusion was achieved in 16 patients (84.2%) and 3 patients (15.8%), respectively. Of the 19 patients, 16 (84.2%) were followed angiographically for a median of 38.5 months (range 16-72 months). None demonstrated recanalization of the aneurysm requiring additional treatment. In 15 patients (78.9%) the final outcome was good (modified Rankin scale, mRS, score 0-2), and 3 patients (15.8%) died or suffered severe disability (mRS score 4-6). None of 18 patients who were followed clinically for a median of 39.5 months (range 17-84 months) experienced rebleeding.
Conclusion: Even tiny ruptured ACoA aneurysms can be safely treated by EVT by expert neurointerventionalists using advanced techniques.
Figures
Similar articles
-
Treatment of basilar artery bifurcation aneurysms by using Guglielmi detachable coils: a 6-year experience.J Neurosurg. 1999 May;90(5):843-52. doi: 10.3171/jns.1999.90.5.0843. J Neurosurg. 1999. PMID: 10223449
-
Guglielmi detachable coil treatment of ruptured saccular cerebral aneurysms: retrospective review of a 10-year single-center experience.AJNR Am J Neuroradiol. 2003 Mar;24(3):526-33. AJNR Am J Neuroradiol. 2003. PMID: 12637310 Free PMC article.
-
Aneurysmal subarachnoid hemorrhage in patients with Hunt and Hess grade 4 or 5: treatment using the Guglielmi detachable coil system.AJNR Am J Neuroradiol. 2003 Apr;24(4):585-90. AJNR Am J Neuroradiol. 2003. PMID: 12695185 Free PMC article.
-
Selection of cerebral aneurysms for treatment using Guglielmi detachable coils: the preliminary University of Illinois at Chicago experience.Neurosurgery. 1998 Dec;43(6):1281-95; discussion 1296-7. doi: 10.1097/00006123-199812000-00011. Neurosurgery. 1998. PMID: 9848841 Review.
-
Complex intracranial aneurysms: combined operative and endovascular approaches.Neurosurgery. 1998 Dec;43(6):1304-12; discussion 1312-3. doi: 10.1097/00006123-199812000-00020. Neurosurgery. 1998. PMID: 9848843 Review.
Cited by
-
AngioSuite-Assisted Volume Calculation and Coil Use Prediction in the Endovascular Treatment of Tiny Volume Intracranial Aneurysms.Biomed Res Int. 2021 Jul 29;2021:5514608. doi: 10.1155/2021/5514608. eCollection 2021. Biomed Res Int. 2021. PMID: 34368348 Free PMC article.
-
The combinational use of dual microcatheter technique and new hypersoft helical coil for endovascular treatment of tiny intracranial aneurysm with difficult geometry.Interv Neuroradiol. 2016 Feb;22(1):18-25. doi: 10.1177/1591019915609124. Epub 2015 Oct 27. Interv Neuroradiol. 2016. PMID: 26508090 Free PMC article.
-
Endovascular treatment of ruptured tiny aneurysms.J Cerebrovasc Endovasc Neurosurg. 2019 Jun;21(2):67-76. doi: 10.7461/jcen.2019.21.2.67. Epub 2019 Jun 30. J Cerebrovasc Endovasc Neurosurg. 2019. PMID: 31886142 Free PMC article.
-
Stent-assisted embolization of wide-neck anterior communicating artery aneurysms: review of 21 consecutive cases.AJNR Am J Neuroradiol. 2009 Sep;30(8):1502-6. doi: 10.3174/ajnr.A1618. Epub 2009 May 20. AJNR Am J Neuroradiol. 2009. PMID: 19461055 Free PMC article.
-
Stand-alone coil embolization of anterior communicating artery aneurysms: Efficacy and technical issues.Neuroradiol J. 2016 Oct;29(5):361-7. doi: 10.1177/1971400916665388. Epub 2016 Aug 16. Neuroradiol J. 2016. PMID: 27531863 Free PMC article.
References
-
- Kassell NF, Torner JC, Haley EC, Jr, Jane JA, Adams HP, Kongable GL. The International Cooperative Study on the Timing of Aneurysm Surgery. Part 1: Overall management results. J Neurosurg. 1990;73:18–36. - PubMed
-
- Yasargil MG. Microneurosurgery, vol II. New York: Thieme; 1984. pp. 169–184.
-
- Kazekawa K, Tsutsumi M, Aikawa H, et al. Endovascular treatment of anterior cerebral artery aneurysms using Guglielmi detachable coils: mid-term clinical evaluation. Radiat Med. 2002;20:291–297. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
