

Diffusion of surgical innovation among patients with kidney cancer
- PMID: 18330868
- PMCID: PMC2650731
- DOI: 10.1002/cncr.23372
Diffusion of surgical innovation among patients with kidney cancer
Abstract
Background: Despite their potential benefits to patients with kidney cancer, the adoption of partial nephrectomy and laparoscopy has been gradual and asymmetric. To clarify whether this trend reflects differences in kidney cancer patients or differences in surgeon practice styles, the authors compared the magnitude of surgeon-attributable variance in the use of partial nephrectomy and laparoscopic radical nephrectomy with that attributable to patient and tumor characteristics.
Methods: By using linked Surveillance, Epidemiology, and End Results-Medicare data, the authors identified a cohort of 5483 Medicare beneficiaries who underwent surgery for kidney cancer between 1997 and 2002. Two primary outcomes were defined: 1) the use of partial nephrectomy and (2) the use of laparoscopy among patients undergoing radical nephrectomy. By using multilevel models, surgeon- and patient-level contributions to observed variations in the use of partial nephrectomy and laparoscopic radical nephrectomy were estimated.
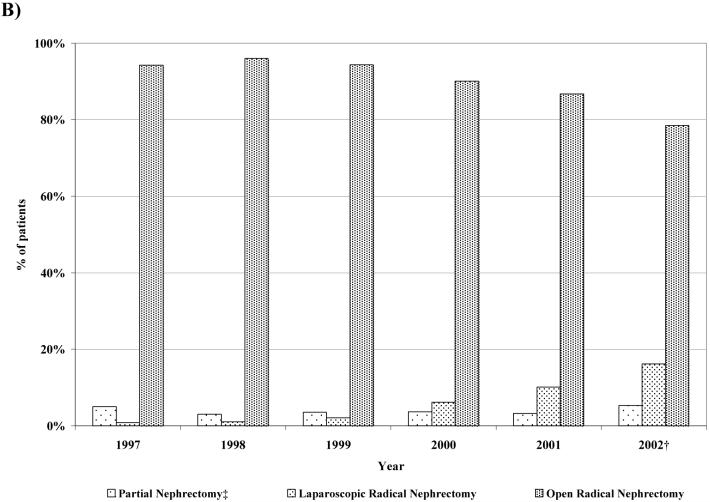
Results: Of the 5483 cases identified, 611 (11.1%) underwent partial nephrectomy (43 performed laparoscopically), and 4872 (88.9%) underwent radical nephrectomy (515 performed laparoscopically). After adjusting for patient demographics, comorbidity, tumor size, and surgeon volume, the surgeon-attributable variance was 18.1% for partial nephrectomy and 37.4% for laparoscopy. For both outcomes, the percentage of total variance attributable to surgeon factors was consistently higher than that attributable to patient characteristics.
Conclusions: For many patients with kidney cancer, the surgery provided depends more on their surgeon's practice style than on the characteristics of the patient and his or her disease. Consequently, dismantling barriers to surgeon adoption of partial nephrectomy and laparoscopy is an important step toward improving the quality of care for patients with early-stage kidney cancer.
Figures

Comment in
-
Barriers to the diffusion of advanced surgical techniques.Cancer. 2008 Apr 15;112(8):1646-9. doi: 10.1002/cncr.23369. Cancer. 2008. PMID: 18300242 No abstract available.
References
-
- Novick AC. Laparoscopic and partial nephrectomy. Clin Cancer Res. 2004;10:6322S–6327S. - PubMed
-
- Miller DC, Wei JT, Dunn RL, Hollenbeck BK. Trends in the diffusion of laparoscopic nephrectomy. JAMA. 2006;295:2480–2482. - PubMed
-
- Miller DC, Hollingsworth JM, Hafez KS, Daignault S, Hollenbeck BK. Partial nephrectomy for small renal masses: an emerging quality of care concern? J Urol. 2006;175:853–857. - PubMed
-
- Miller DC, Taub DA, Dunn RL, Wei JT, Hollenbeck BK. Laparoscopy for renal cell carcinoma: diffusion versus regionalization? J Urol. 2006;176:1102–1106. - PubMed
-
- Permpongkosol S, Bagga HS, Romero FR, Solomon SB, Kavoussi LR. Trends in the operative management of renal tumors over a 14-year period. BJU Int. 2006;98:751–755. - PubMed
