

Obesity and central obesity as risk factors for incident dementia and its subtypes: a systematic review and meta-analysis
- PMID: 18331422
- PMCID: PMC4887143
- DOI: 10.1111/j.1467-789X.2008.00473.x
Obesity and central obesity as risk factors for incident dementia and its subtypes: a systematic review and meta-analysis
Erratum in
- Obes Rev. 2008 May;9(3):267
Abstract
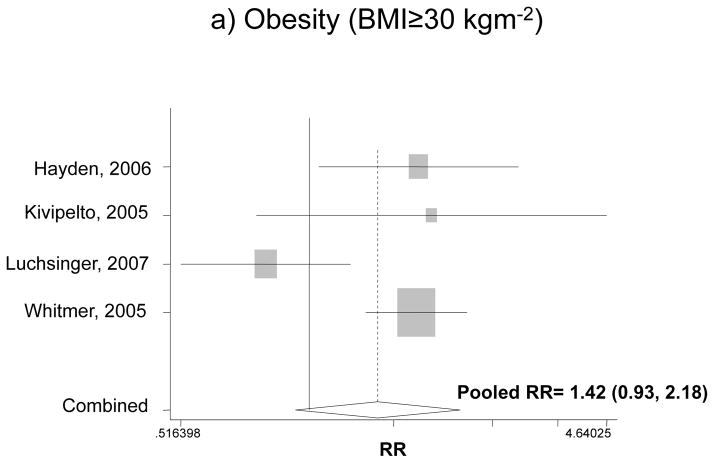
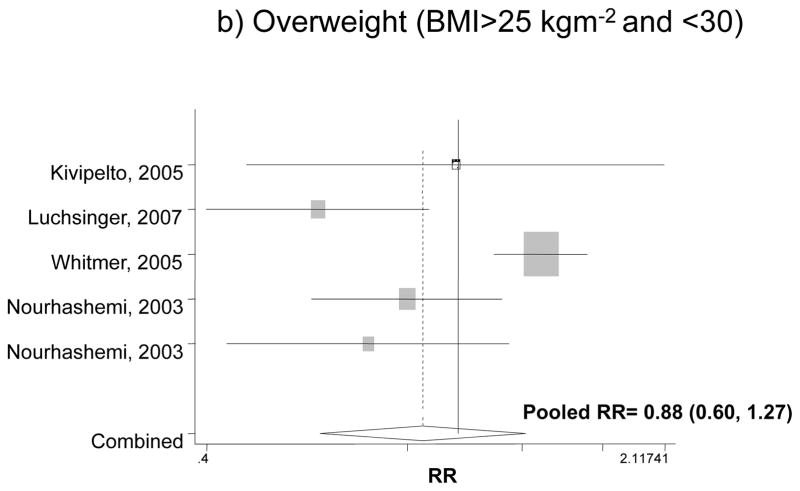
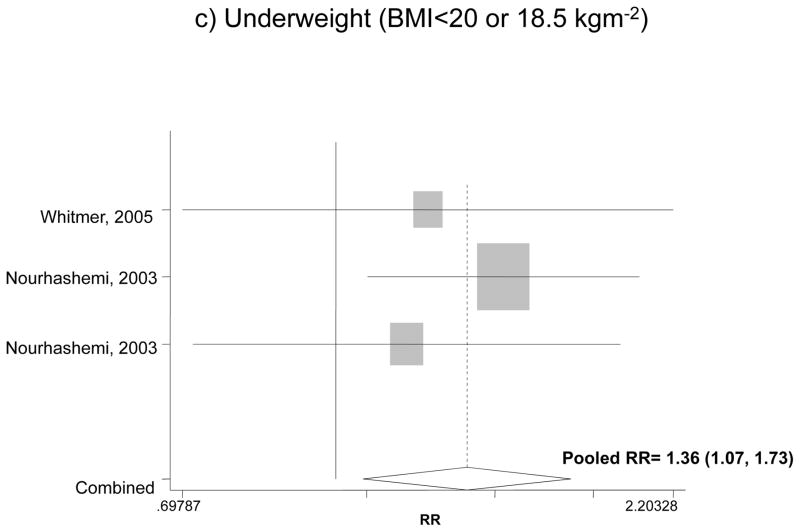
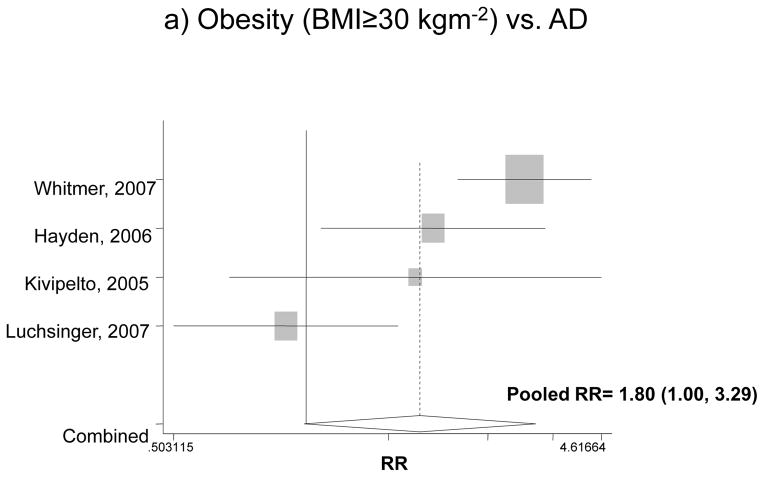
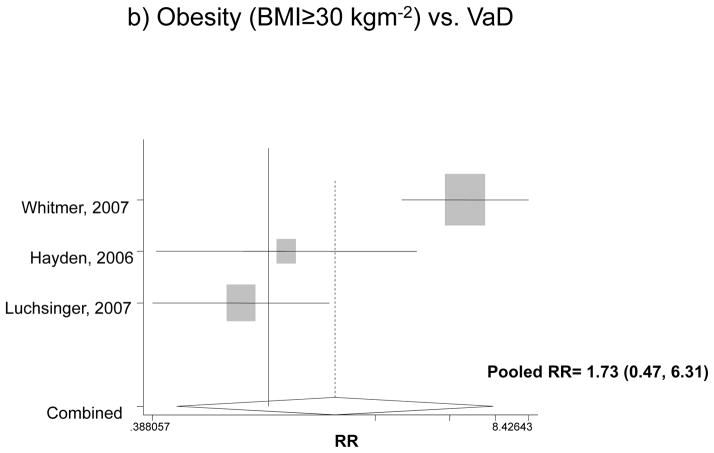
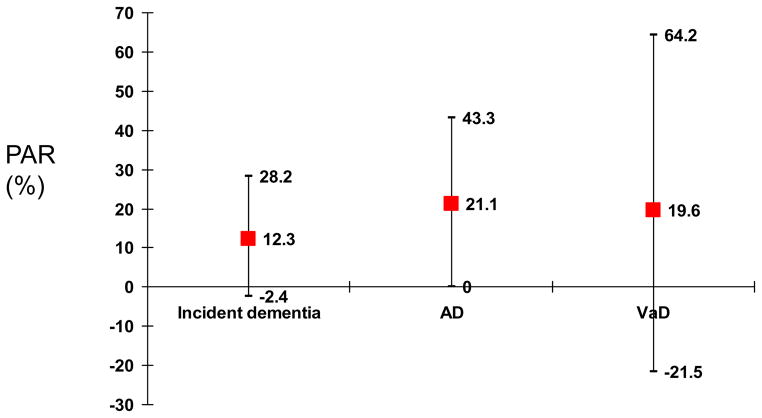
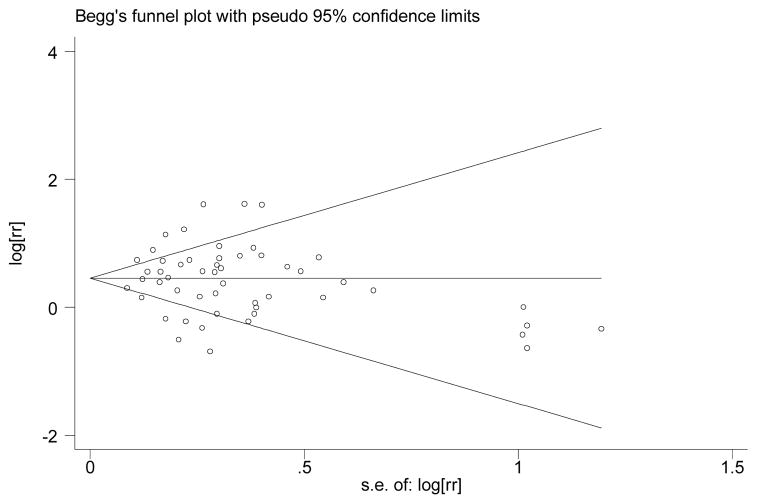
While dementia affects 6-10% of persons 65 years or older, industrialized countries have witnessed an alarming rise in obesity. However, obesity's influence on dementia remains poorly understood. We conducted a systematic review and meta-analysis. PUBMED search (1995-2007) resulted in 10 relevant prospective cohort studies of older adults (40-80 years at baseline) with end points being dementia and predictors including adiposity measures, such as body mass index (BMI) and waist circumference (WC). There was a significant U-shaped association between BMI and dementia (P = 0.034), with dementia risk increased for obesity and underweight. Pooled odds ratios (OR) and 95% confidence intervals (CI) for underweight, overweight and obesity compared with normal weight in relation to incident dementia were: 1.36 (1.07, 1.73), 0.88 (0.60, 1.27) and 1.42 (0.93, 2.18) respectively. Pooled ORs and 95% CI for obesity and incident Alzheimer's disease (AD) and vascular dementia were 1.80 (1.00, 3.29) vs. 1.73 (0.47, 6.31) and were stronger in studies with long follow-up (>10 years) and young baseline age (<60 years). Weight gain and high WC or skin-fold thickness increased risks of dementia in all included studies. The meta-analysis shows a moderate association between obesity and the risks for dementia and AD. Future studies are needed to understand optimal weight and biological mechanisms.
Figures
Comment in
-
Weight loss occurs over a decade prior to dementia diagnosis: comment on meta-analysis of obesity as a risk factor for dementia and its subtypes.Obes Rev. 2008 Nov;9(6):631-2; author reply 633-4. doi: 10.1111/j.1467-789X.2008.00519.x. Epub 2008 Sep 17. Obes Rev. 2008. PMID: 18801008 No abstract available.
References
-
- Hendrie HC. Epidemiology of dementia and Alzheimer’s disease. Am J Geriatr Psychiatry. 1998;6:S3–18. - PubMed
-
- Centers of Disease Control and Prevention. Death: preliminary data 2003. Natl Vital Stat Rep. 2005:53. - PubMed
-
- Dewey ME, Saz P. Dementia, cognitive impairment and mortality in persons aged 65 and over living in the community: a systematic review of the literature. Int J Geriatr Psychiatry. 2001;16:751–61. - PubMed
-
- Abate C, Ferrari-Ramondo V, Di Iorio A. Risk factors for cognitive disorders in the elderly: A review. Archives of Gerontology and Geriatrics. 1998;(suppl 6):7–15.
-
- Clarke R, Smith AD, Jobst KA, Refsum H, Sutton L, Ueland PM. Folate, vitamin B12, and serum total homocysteine levels in confirmed Alzheimer disease. Arch Neurol. 1998;55:1449–55. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
