

Pharmacodynamic analysis and clinical trial of amoxicillin sprinkle administered once daily for 7 days compared to penicillin V potassium administered four times daily for 10 days in the treatment of tonsillopharyngitis due to Streptococcus pyogenes in children
- PMID: 18332170
- PMCID: PMC2443932
- DOI: 10.1128/AAC.00132-07
Pharmacodynamic analysis and clinical trial of amoxicillin sprinkle administered once daily for 7 days compared to penicillin V potassium administered four times daily for 10 days in the treatment of tonsillopharyngitis due to Streptococcus pyogenes in children
Abstract
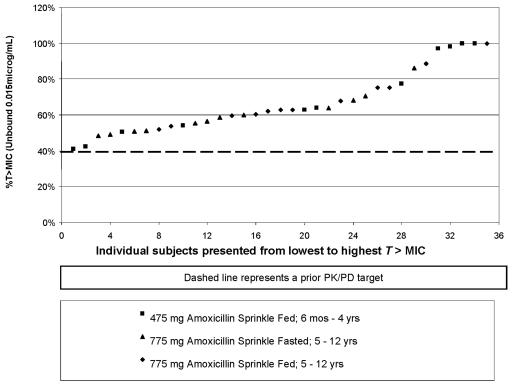
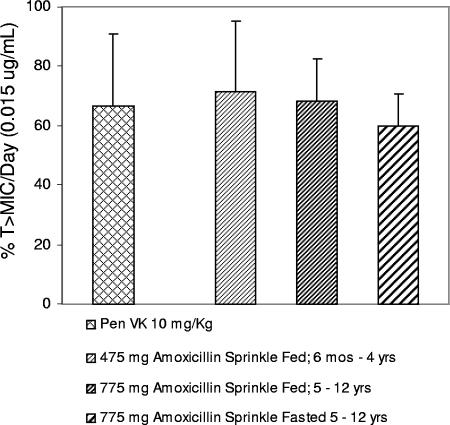
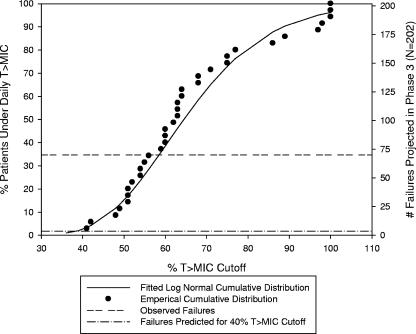
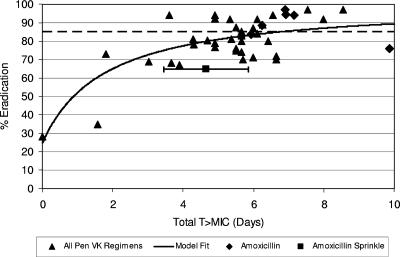
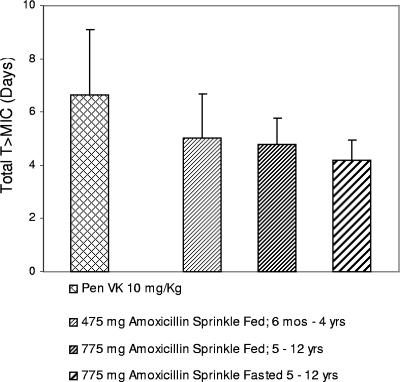
An a priori pharmacokinetic/pharmacodynamic (PK/PD) target of 40% daily time above the MIC (T >MIC; based on the MIC(90) of 0.06 microg/ml for Streptococcus pyogenes reported in the literature) was shown to be achievable in a phase 1 study of 23 children with a once-daily (QD) modified-release, multiparticulate formulation of amoxicillin (amoxicillin sprinkle). The daily T >MIC achieved with the QD amoxicillin sprinkle formulation was comparable to that achieved with a four-times-daily (QID) penicillin VK suspension. An investigator-blinded, randomized, parallel-group, multicenter study involving 579 children 6 months to 12 years old with acute streptococcal tonsillopharyngitis was then undertaken. Children were randomly assigned 1:1 to receive either the amoxicillin sprinkle (475 mg for ages 6 months to 4 years, 775 mg for ages 5 to 12 years) QD for 7 days or 10 mg/kg of body weight of penicillin VK QID for 10 days (up to the maximum dose of 250 mg QID). Unexpectedly, the rates of bacteriological eradication at the test of cure were 65.3% (132/202) for the amoxicillin sprinkle and 68.0% (132/194) for penicillin VK (95% confidence interval, -12.0% to 6.6%). Thus, neither antibiotic regimen met the minimum criterion of > or =85% eradication ordinarily required by the U.S. FDA for first-line treatment of tonsillopharyngitis due to S. pyogenes. The results of subgroup analyses across demographic characteristics and current infection characteristics and by age/weight categories were consistent with the primary-efficacy result. The clinical cure rates for amoxicillin sprinkle and penicillin VK were 86.1% (216/251) and 91.9% (204/222), respectively (95% confidence interval, -11.6% to -0.4%). The results of a post hoc PD analysis suggested that a requirement for 60% daily T >MIC(90) more accurately predicted the observed high failure rates for bacteriologic eradication with the amoxicillin sprinkle and penicillin VK suspension studied. Based on the association between longer treatment courses and maximal bacterial eradication rates reported in the literature, an alternative composite PK/PD target taking into consideration the duration of therapy, or total T >MIC, was considered and provides an alternative explanation for the observed failure rate of amoxicillin sprinkle.
Figures
References
-
- Aguilar, A., J. C. Tinoco, M. Macias, L. Huicho, J. Levy, H. Trujillo, P. Lopez, M. Pereira, S. Maqbool, Z. A. Bhutta, R. A. Sacy, and S. Deacon. 2000. Clinical and bacteriologic efficacy of amoxycillin b.d. (45 mg/kg/day) versus amoxycillin t.d.s (40 mg/kg/day) in children with group A beta-hemolytic streptococcal tonsillopharyngitis. J. Chemother. 12:396-405. - PubMed
-
- Bisno, A. L., M. A. Gerber, J. M. Gwaltney, Jr., E. L. Kaplan, and R. H. Schwartz. 2002. Practice guidelines for the diagnosis and management of group A streptococcal pharyngitis. Clin. Infect. Dis. 35:113-125. - PubMed
-
- Block, S. L. 2007. Safety and efficacy of amoxicillin PULSYS 775 mg PO QD for 10 days compared to penicillin VK 250 mg QID for 10 days in the treatment of Streptococcus pyogenes tonsillitis and/or pharyngitis in adolescents and adults, abstr. 199a. Abstr. 45th Ann. Meet. Infect. Dis. Soc. Am., San Diego, CA, 4 to 7 October 2007.
-
- Block, S. L., J. A. Hedrick, and R. D. Tyler. 1992. Comparative study of the effectiveness of cefixime and penicillin V for the treatment of streptococcal pharyngitis in children and adolescents. Pediatr. Infect. Dis. J. 11:919-925. - PubMed
-
- Bradley, J. S., M. N. Dudley, and G. L. Drusano. 2003. Predicting efficacy of antiinfectives with pharmacodynamics and Monte Carlo simulation. Pediatr. Infect. Dis. J. 22:982-992. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
