

Pancreatic resection for metastatic melanoma
- PMID: 18332980
- PMCID: PMC2020574
- DOI: 10.1080/13651820310015284
Pancreatic resection for metastatic melanoma
Abstract
Background: The pancreas is an occasional site of metastases from melanoma. It may be the only location of metastatic disease, but more often the melanoma metastasis to other organs as well. Treatment options are somewhat limited, and the role of operative treatment is poorly defined.
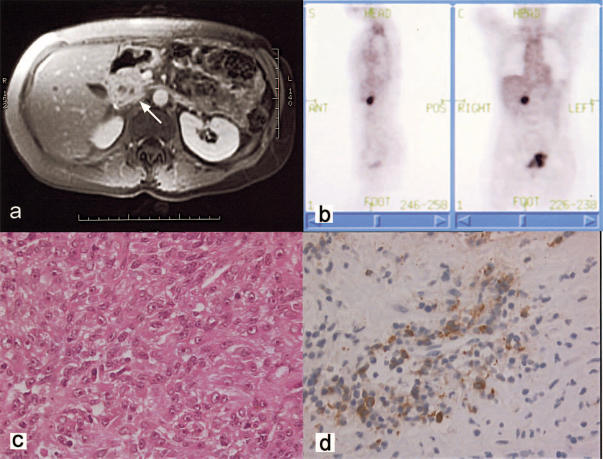
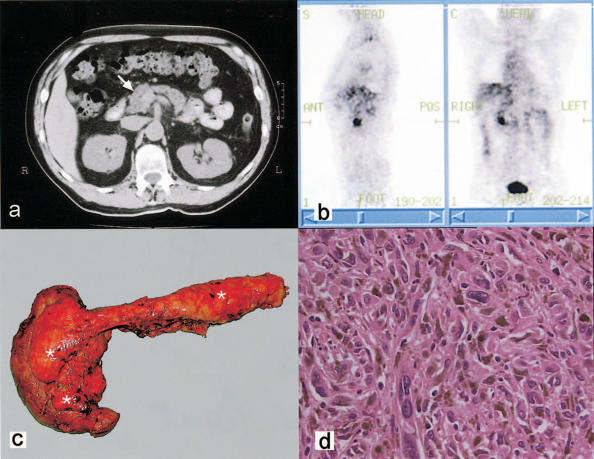
Case outlines: Two patients presenting with abdominal pain were found to have pancreatic lesions. A 45-year-old woman had a pylorus-preserving pancreatoduodenectomy for a mass in the head of pancreas; concurrent liver nodules were treated by segmental liver resection. A 55-year-old man had a total pancreatectomy for multiple pancreatic tumours. Both patients gave a history of ocular melanoma, diagnosed >10 years previously. They had no evidence of malignancy elsewhere. Histology of resected specimens confirmed metastatic melanoma with features consistent with an ocular primary. All resection margins were clear of malignancy, and no lymph node metastases were detected. At 6 months follow-up there were no signs of tumour recurrence.
Discussion: Complete surgical resection offers potential cure in selected patients with metastatic melanoma involving the pancreas, when there is no evidence of widespread disease.
Figures
References
-
- Willis RA. Butterworth; London: 1973. The Spread of Tumors in the Human Body3rd edn; pp. 216–17.
-
- Cubilla AL, Fitzgerald PJ. Moosa AR. Willimans & Wilkins; Baltimore: 1980. Surgical pathology of tumors of the exocrine pancreas, Tumors of the Pancreas; pp. 159–63.
-
- Z'Graggen K, Fernandez-del Castillo C, Rattner DW, Sigala H, Warshaw AL. Metastases to the pancreas and their surgical extirpation. Arch Surg 1998;133:413–17; discussion 418–19. - PubMed
-
- Hiotis SP, Klimstra DS, Conlon KC, Brennan MF. Results after pancreatic resection for metastatic lesions. Ann Surg Oncol. 2002;9:675–9. - PubMed
-
- Harrison LE, Merchant N, Cohen AM, Brennan MF. Pancreaticoduodenectomy for nonperiampullary primary tumors. Am J Surg. 1997;174:393–5. - PubMed
LinkOut - more resources
Full Text Sources
