

Controversies in the laparoscopic treatment of hepatic hydatid disease
- PMID: 18333078
- PMCID: PMC2020683
- DOI: 10.1080/13651820410024003
Controversies in the laparoscopic treatment of hepatic hydatid disease
Abstract
Background: Laparoscopic treatment of hydatid disease of the liver can be performed safely in selected patients.
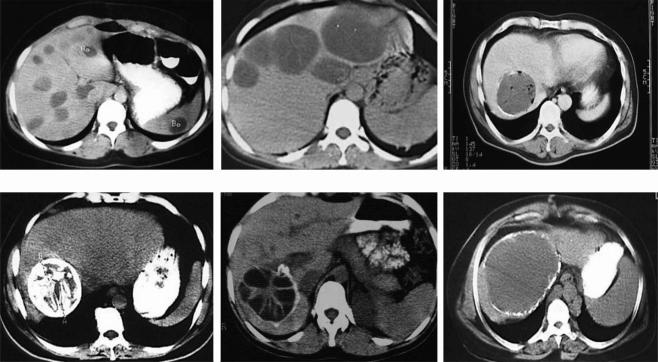
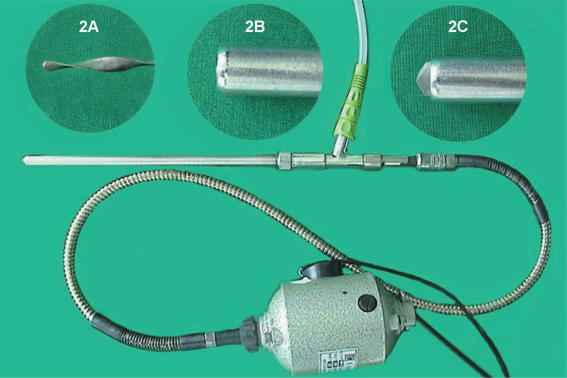
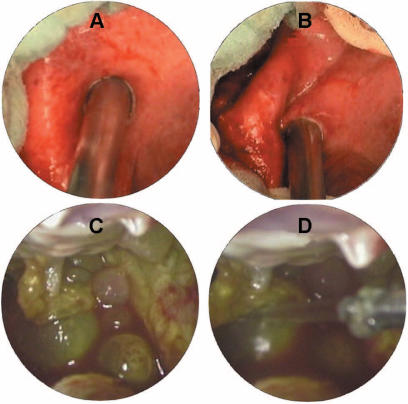
Methods: Six hundred and fifty patients were treated for hydatid disease of the liver between 1980 and 2003 at the Hepatopancreatobiliary Surgery Unit of Istanbul Medical Faculty, Istanbul University. Of these, 60 were treated laparoscopically between 1992 and 2000. A special aspirator-grinder apparatus was used for the evacuation of cyst contents. Ninety-two percent of the cysts were at stages I, II or III according to the ultrasonographic classification of Gharbi.
Results: Conversion to open surgery was necessary in eight patients due to intra-abdominal adhesions or cysts in difficult locations. There was no disease- or procedure-related mortality. Most of the complications were related to cavity infections (13.5%) and external biliary fistulas (11.5%) resulting from communications between the cysts and the biliary tree. There were two recurrences in a follow-up period ranging between 3.5 and 11 years.
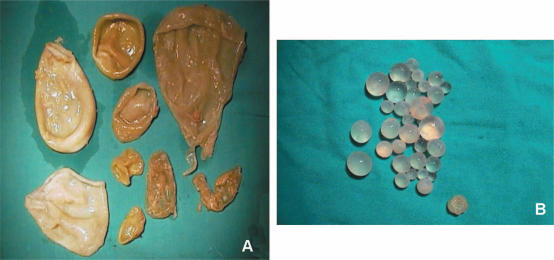
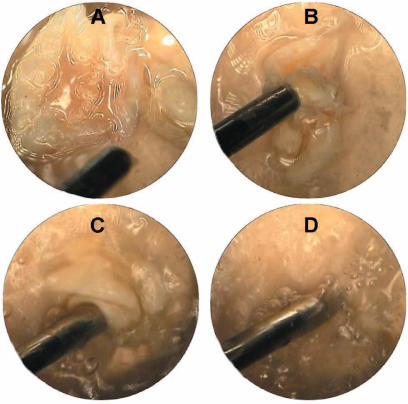
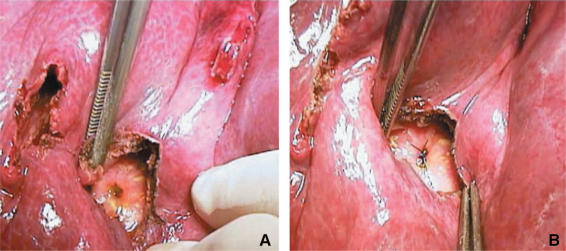
Discussion: Laparoscopic treatment of hydatid disease of the liver is an alternative to open surgery in well-selected patients. Important steps are the evacuation of the cyst contents without spillage, sterilization of the cyst cavity with scolicidal agents and cavity management using classical surgical techniques. Our specially designed aspirator-grinder apparatus was safely used to evacuate the cyst contents without causing any spillage. Knowledge of the relationship of the cyst with the biliary tree is essential in choosing the appropriate patients for the laparoscopic technique. In our experience of 650 cases, the biliary communication rate was as high as 18%; half of these can be detected preoperatively. In the remaining, biliary communications are usually detected during or after surgery. Endoscopic retrograde cholangiopancreatography (ERCP) and sphincterotomy are helpful to overcome this problem. As hydatid disease of the liver is a benign and potentially recurrent disease, we advocate the use of conservative techniques in both laparoscopic and open operations.
Figures
References
-
- Mentes A. Hydatid liver disease: a perspective in treatment. Dig Dis. 1994;12:150–60. - PubMed
-
- Meyers WC, Kim RD, Chari RS. Townsend CM, Beauchamp RD, Evers BM, Mattox KL. WB Saunders; Philadelphia: 2001. Echinococcal cysts, Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice; pp. 1053–5.
-
- Sayek I, Yalin R, Sarac Y. Surgical treatment of hydatid disease of the liver. Arch Surg. 1980;115:847–50. - PubMed
-
- Gharbi HA, Hassine W, Brauner M, Dupuch K. Ultrasound examination of the hydatid liver. Radiology. 1981;139:459–63. - PubMed
-
- Caremani M, Benci A, Maestrini R, Rossi G, Menchetti D. Abdominal cystic hydatid diseases (CHD): classification of sonographic appearance and response to treatment. J Clin Ultrasound. 1996;24:491–500. - PubMed
LinkOut - more resources
Full Text Sources
