

Diagnosis of pancreatic cancer
- PMID: 18333085
- PMCID: PMC2020745
- DOI: 10.1080/13651820500540949
Diagnosis of pancreatic cancer
Abstract
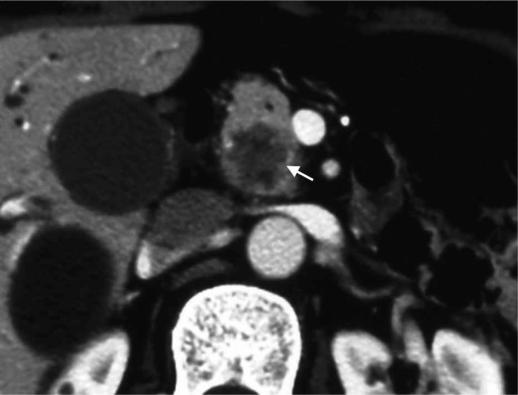
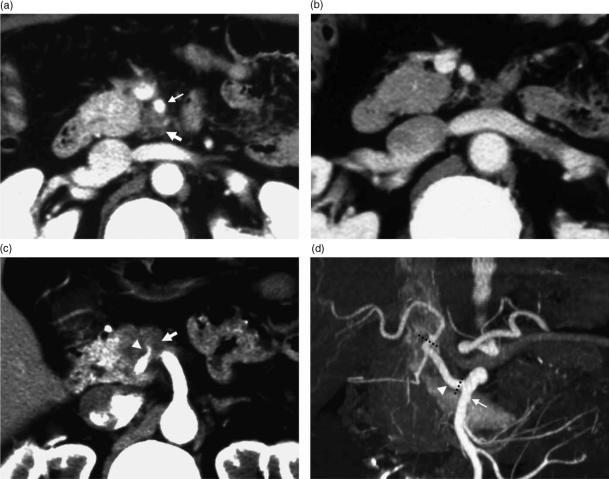
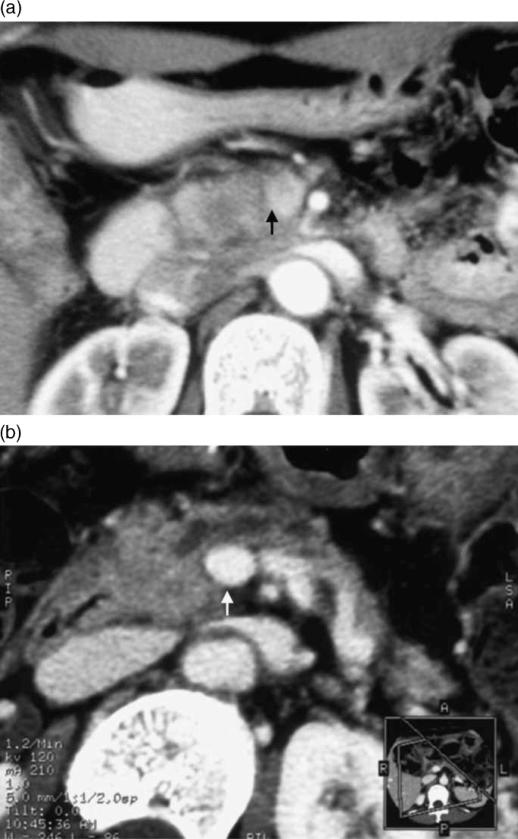
The ability to diagnose pancreatic carcinoma has been rapidly improving with the recent advances in diagnostic techniques such as contrast-enhanced Doppler ultrasound (US), helical computed tomography (CT), enhanced magnetic resonance imaging (MRI), and endoscopic US (EUS). Each technique has advantages and limitations, making the selection of the proper diagnostic technique, in terms of purpose and characteristics, especially important. Abdominal US is the modality often used first to identify a cause of abdominal pain or jaundice, while the accuracy of conventional US for diagnosing pancreatic tumors is only 50-70%. CT is the most widely used imaging examination for the detection and staging of pancreatic carcinoma. Pancreatic adenocarcinoma is generally depicted as a hypoattenuating area on contrast-enhanced CT. The reported sensitivity of helical CT in revealing pancreatic carcinoma is high, ranging between 89% and 97%. Multi-detector-row (MD) CT may offer an improvement in the early detection and accurate staging of pancreatic carcinoma. It should be taken into consideration that some pancreatic adenocarcinomas are depicted as isoattenuating and that pancreatitis accompanied by pancreatic adenocarcinoma might occasionally result in the overestimation of staging. T1-weighted spin-echo images with fat suppression and dynamic gradient-echo MR images enhanced with gadolinium have been reported to be superior to helical CT for detecting small lesions. However, chronic pancreatitis and pancreatic carcinoma are not distinguished on the basis of degree and time of enhancement on dynamic gadolinium-enhanced MRI. EUS is superior to spiral CT and MRI in the detection of small tumors, and can also localize lymph node metastases or vascular tumor infiltration with high sensitivity. EUS-guided fine-needle aspiration biopsy is a safe and highly accurate method for tissue diagnosis of patients with suspected pancreatic carcinoma. (18)F-fluorodeoxyglucose (FDG) positron emission tomography (PET) has been suggested as a promising modality for noninvasive differentiation between benign and malignant lesions. Previous studies reported the sensitivity and specificity of FDG-PET for detecting malignant pancreatic tumors as being 71-100% and 64-90%, respectively. FDG-PET does not replace, but is complementary to morphologic imaging, and therefore, in doubtful cases, the method must be combined with other imaging modalities.
Figures
References
-
- Nakagohri T, Kinoshita T, Konishi M, Inoue K, Takahashi S. Survival benefits of portal vein resection for pancreatic cancer. Am J Surg. 2003;186:149–53. - PubMed
-
- Kobari M, Matsuno S. Staging systems for pancreatic cancer: differences between the Japanese and UICC systems. J Hepatobiliary Pancreat Surg. 1998;5:121–7. - PubMed
-
- Karlson BM, Ekbom A, Lindgren PG, Kallskog V, Rostad J. Abdominal US for diagnosis of pancreatic tumor: prospective cohort analysis. Radiology. 1999;213:107–11. - PubMed
-
- Rickes S, Unkrodt K, Neye H, Okran KW, Wermke W. Differentiation of pancreatic tumours by conventional ultrasound, unenhanced and echo-enhanced power Doppler sonography. Scand J Gastroenterol. 2002;37:1313–20. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
