

Mirizzi's syndrome--results from a large western experience
- PMID: 18333104
- PMCID: PMC2020759
- DOI: 10.1080/13651820600840082
Mirizzi's syndrome--results from a large western experience
Abstract
Background: This paper reports a series of patients with Mirizzi's syndrome (MS) who were managed at our institution over an 11-year (1994-2005) period.
Methods: Retrospective case note study of patients with a definitive or possible diagnosis of MS stated in radiology reports were identified using the hospital's radiology computer coding system.
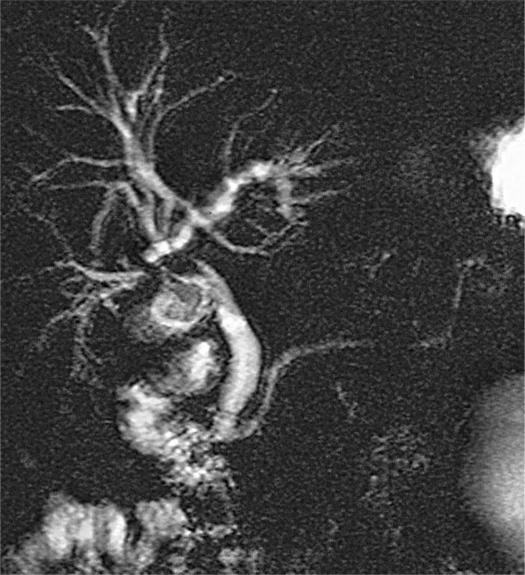
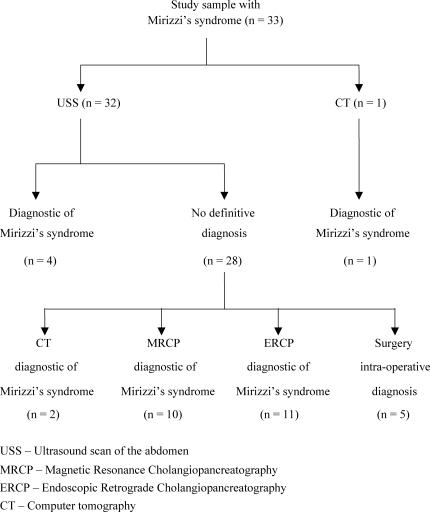
Results: 33 patients were identified with a median age of diagnosis of 70 (35-90) years and male to female ratio of 15:18. Liver function tests were deranged in all patients. Pre-operative radiological diagnosis was achieved in 28 patients: ultrasound scan (n = 4), computer tomography (n = 3), magnetic resonance cholangiopancreatography (n = 10) and endoscopic retrograde cholangiopancreatography (n = 11). Five patients were diagnosed intra-operatively. Type I MS was reported in 27 patients. Laparoscopic cholecystectomy was attempted in 18 patients with 6 being converted to open cholecystectomy. Six patients had biliary stent insertion only and 3 were conservatively managed. Six patients had type II MS, 4 were treated with open cholecystectomy and Roux-en-Y hepaticojejunostomy, 1 underwent an open subtotal cholecystectomy with fistula closure and 1 had percutaneous biliary stent insertion only. The median follow-up period was 2 (1-7) months (n = 18). 10 patients are currently under follow-up. Overall morbidity was 27% (n = 8) and mortality was 7% (n = 2).
Conclusion: Pre-operative diagnosis of MS can be achieved using MRCP. Laparoscopic cholecystectomy for type I MS is a safe option and type II MS can be treated with Roux-en-Y hepaticojejunostomy or subtotal cholecystectomy with fistula closure.
Figures

References
-
- Mirizzi PL. Syndrome del conducto hepatico. Journal International du Chirurgie. 1948;8:731–77.
-
- McSherry CK, Ferstenberg H, Virshup M. The Mirizzi's syndrome: Suggested classification and surgical therapy. Surg Gastroenterol. 1982;1:219–25.
-
- Csendes A, Carlos Diaz , Burdiles P, Maluenda F, Nava O. Mirizzi's syndrome and cysto-biliary fistula: a unifying classification. Br J Surg. 1989;76:1139–43. - PubMed
-
- Mishra MC, Vashishtha S, Tandon R. Bilio-biliary fistula: pre-operative diagnosis and management implications. Surgery. 1990;108:835–9. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
