

Minimising blood loss and transfusion requirements in hepatic resection
- PMID: 18333146
- PMCID: PMC2023906
- DOI: 10.1080/136518202753598672
Minimising blood loss and transfusion requirements in hepatic resection
Abstract
Background: Substantial blood loss and the requirement for blood transfusion remain major considerations for hepatic surgeons. We analysed the impact of a systematic protocol aimed at reducing intraoperative blood loss and homologous blood (HB) transfusion associated with hepatic resection.
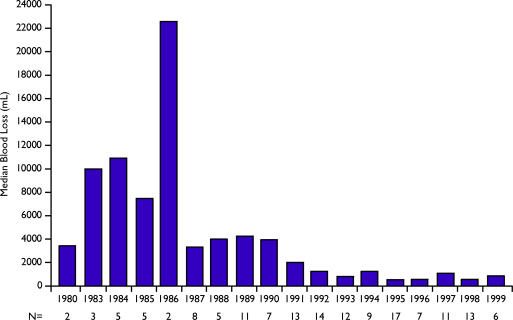
Methods: Prospective clinical data were collected from 151 elective liver resections performed during the period between 1980 and 1999. Further data directly related to blood loss and anaesthesia were retrospectively collected from the anaesthetic intra-operative record. Strategies implemented in 1991 included preoperative autologous blood donation, low central venous pressure anaesthesia, aprotinin administration, ultrasonic dissection, hepatic vascular inflow occlusion and a Cell Saver. Blood loss and transfusion requirements were studied before and after the implementation of these strategies.
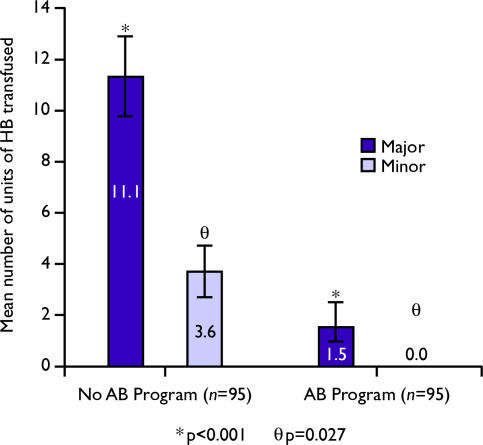
Results: There was no difference in the patient demographics, indications for operation or the scope of resections in the two time periods evaluated. Blood-saving strategies resulted in decreased estimated blood loss (4500 mL vs. 1000 mL p<0.001). In addition, the number of patients requiring transfusion decreased (91.8% vs. 25.5% respectively, p<0.001) and the mean number of units of HB transfusion was lower (I 3.7 vs. 2.3, p<0.001). Morbidity and mortality were also decreased (57.1% vs. 25.5%, p<0.001 and 10.2% and 4.9% p<0.001, respectively). No complications directly referrable to low CVP anesthesia were identified.
Conclusion: Systematic implementation of strategies designed to control blood loss are effective and may reduce morbidity and mortality associated with hepatic resections.
Figures
Comment in
-
Integrated blood conservation programme to minimise blood loss and transfusion requirements in hepatic resection.HPB (Oxford). 2002;4(4):199-200; author reply 201. doi: 10.1080/13651820260503891. HPB (Oxford). 2002. PMID: 18332956 Free PMC article. No abstract available.
References
-
- Steele G, Bleday R, Mayer RJ, Lindblad A, Petrelli N, Weaver D. A prospective evaluation of hepatic resection for colorectal carcinoma metastases to the liver: Gastrointestinal Tumor Study Group Protocol 6584. J Clin Oncol. 1991;9:1105–12. - PubMed
-
- Little JM. Hepatic secondaries: minimal tumor and resectable tumor. World J Surg. 1984;8:753–6. - PubMed
-
- Van Ooijen B, Wiggers T, Meijer S, et al. Hepatic resectionfor colorectal metastases in the Netherlands: a multi-institutional 10-year study. Cancer. 1984;70:28–34. - PubMed
LinkOut - more resources
Full Text Sources
