

Staging systems in hepatocellular carcinoma
- PMID: 18333159
- PMCID: PMC2023920
- DOI: 10.1080/13651820410024058
Staging systems in hepatocellular carcinoma
Abstract
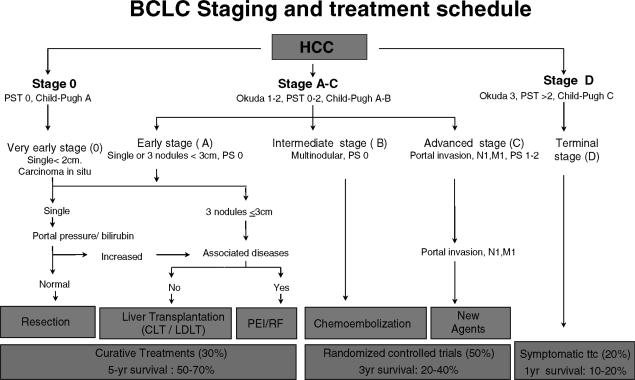
Staging systems are key to predict the prognosis of patients with cancer, to stratify the patients according to prognostic variables in the setting of clinical trials, to allow the exchange of information among researchers, and finally to guide the therapeutic approach. The current knowledge of the disease, however, prevents recommendation of a staging system that can be used world-wide. The conventional staging systems for hepatocellular carcinoma (HCC), such as the Okuda stage or the TNM stage have shown important limitations in classifying patients. Several new systems have been proposed recently, and only three of them have been validated at this point. The BCLC staging classification links the stage of the disease to a specific treatment strategy. The JIS score has been proposed and used in Japan, although it needs Western validation. The CLIP score is used in patients with advanced tumors. Several reasons explain the difficulty in identifying a world-wide system. First, HCC is a complex neoplasm inserted on a pre-neoplastic cirrhotic liver, and thus variables of both diseases leading to death should be taken into account. Second, the disease is very heterogeneous around the world, and this reflects different underlying epidemiological backgrounds and risk factors. Third, HCC is the sole cancer treated by transplantation in a small proportion of patients. Fourth, only around 20% of the cases are currently treated by surgery, thus precluding the wide use of pathology-based systems, such as TNM. Finally, the potential relevance of a molecular signature identified in terms of outcome prediction is unknown, and further research is needed to obtain this valuable biological information that may aid in classifying the patients.
Figures
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Estimating the world cancer burden: GLOBOCAN 2000. Int J Cancer. 2001;94:153–6. - PubMed
-
- Tanaka Y, Hanada K, Mizokami M, Yeo AE, Shih JW, Gojobori T, et al. A comparison of the molecular clock of hepatitis C virus in the United States and Japan predicts that hepatocellular carcinoma incidence in the United States will increase over the next two decades. Proc Natl Acad Sci USA. 2002;99:15584–9. - PMC - PubMed
-
- Fattovich G, Giustina G, Degos F, Tremolada F, Diodati G, Almasio P, et al. Morbidity and mortality in compensated cirrhosis type C: a retrospective follow-up study of 384 patients. Gastroenterology. 1997;112:463–72. - PubMed
-
- Llovet JM, Burroughs A, Bruix J. Hepatocellular carcinoma. Lancet. 2003;362:1907–17. - PubMed
-
- Liaw YF, Tai DI, Chu CM, Lin DY, Sheen IS, Chen TJ, et al. Early detection of hepatocellular carcinoma in patients with chronic type B hepatitis. A prospective study. Gastroenterology. 1986;90:263–7. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
