

Surgical management of hilar cholangiocarcinoma: the Nagoya experience
- PMID: 18333203
- PMCID: PMC2043097
- DOI: 10.1080/13651820500373010
Surgical management of hilar cholangiocarcinoma: the Nagoya experience
Abstract
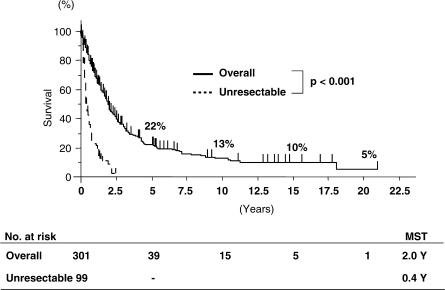
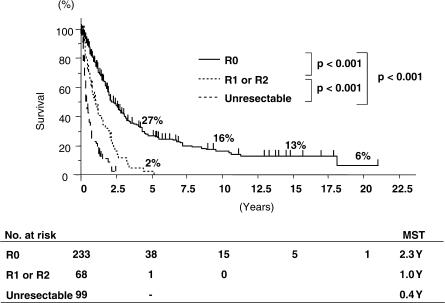
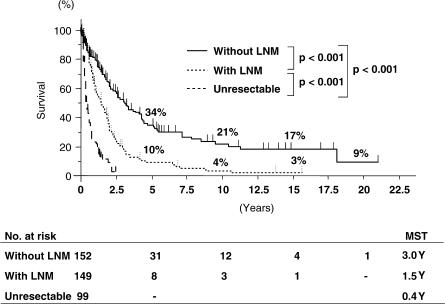
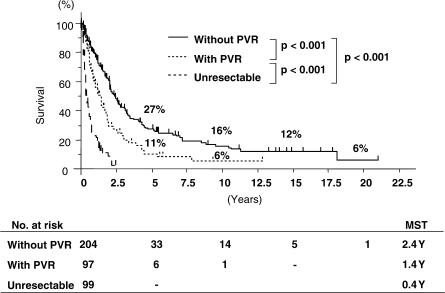
Of 400 patients with hilar cholangiocarcinoma who were treated at Nagoya University Hospital from 1977 to 2004, 301 (75%) underwent surgical resection. Most patients underwent major hepatectomy with extrahepatic bile duct resection. The overall mortality rate was 7.6% but had decreased to 2.5% in the last 5 years (p=0.007). The overall survival rates at 5, 10 and 15 years were 22%, 13% and 10%, respectively. The survival rates of 233 patients undergoing R0 resection were 27%, 16% and 13%, respectively. R1 or R2 resection, lymph node metastasis and portal vein involvement were significant negative prognostic factors, although survival was better than in patients with unresected tumours. The results show that aggressive surgical treatment of hilar cholangiocarcinoma offers good outcomes with an acceptable mortality rate.
Figures
References
-
- Tashiro S, Tsuji T, Kanemitsu K, Kamimoto Y, Hiraoka T, Miyauchi Y. Prolongation of survival for carcinoma at the hepatic duct confluence. Surgery. 1993;113:270–8. - PubMed
-
- Nimura Y, Hayakawa N, Kamiya J, Kondo S, Shionoya S. Hepatic segmentectomy with caudate lobe resection for bile duct carcinoma of the hepatic hilus. World J Surg. 1990;14:535–44. - PubMed
-
- Nimura Y, Hayakawa N, Kamiya J, Maeda S, Kondo S, Yasui A, et al. Combined portal vein and liver resection for carcinoma of the biliary tract. Br J Surg. 1991;78:727–31. - PubMed
LinkOut - more resources
Full Text Sources
