

The 6-plus-person lift transfer technique compared with other methods of spine boarding
- PMID: 18335007
- PMCID: PMC2231400
- DOI: 10.4085/1062-6050-43.1.6
The 6-plus-person lift transfer technique compared with other methods of spine boarding
Abstract
Context: To achieve full spinal immobilization during on-the-field management of an actual or potential spinal injury, rescuers transfer and secure patients to a long spine board. Several techniques can be used to facilitate this patient transfer.
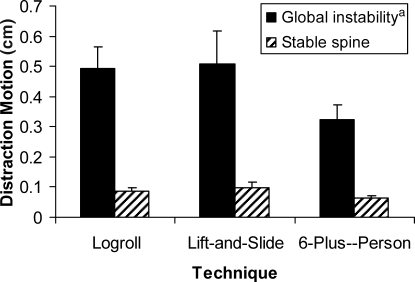
Objective: To compare spinal segment motion of cadavers during the execution of the 6-plus-person (6+) lift, lift-and-slide (LS), and logroll (LR) spine-board transfer techniques.
Design: Crossover study.
Setting: Laboratory.
Patients or other participants: Eight medical professionals (1 woman, 7 men) with 5 to 32 years of experience were enlisted to help carry out the transfer techniques. In addition, test conditions were performed on 5 fresh cadavers (3 males, 2 females) with a mean age of 86.2 +/- 11.4 years.
Main outcomes measure(s): Three-dimensional angular and linear motions initially were recorded during execution of transfer techniques, initially using cadavers with intact spines and then after C5-C6 spinal segment destabilization. The mean maximal linear displacement and angular motion obtained and calculated from the 3 trials for each test condition were included in the statistical analysis.
Results: Flexion-extension angular motion, as well as anteroposterior and distraction-compression linear motion, did not vary between the LR and either the 6+ lift or LS. Compared with the execution of the 6+ lift and LS, the execution of the LR generated significantly more axial rotation (P = .008 and .001, respectively), more lateral flexion (P = .005 and .003, respectively), and more medial-lateral translation (P = .003 and .004, respectively).
Conclusions: A small amount of spinal motion is inevitable when executing spine-board transfer techniques; however, the execution of the 6+ lift or LS appears to minimize the extent of motion generated across a globally unstable spinal segment.
Keywords: lift-and-slide transfer technique; logroll transfer technique; prehospital care; spinal immobilization; spine injuries.
Figures






References
-
- Poonnoose P.M, Ravichandran G, McClelland M.R. Missed and mismanaged injuries of the spinal cord. J Trauma. 2002;53(2):314–320. - PubMed
-
- Krohmer J.R, Marshall L, Newell L.D, American College of Emergency Physicians, editors. EMT – Basic Field Care: A Case-Based Approach. St Louis, MO: Mosby Inc; 1999. pp. 153,510–513,521–525.
-
- De Lorenzo R.A, Olson J.E, Boska M, et al. Optimal positioning for cervical immobilization. Ann Emerg Med. 1996;28(3):301–308. - PubMed
-
- Suter R.E, Tighe T.V, Sartori J, Reed K. Thoraco-lumbar spinal instability during variations of the log-roll maneuver. Prehosp Disaster Med. 1992;7:133–138.
-
- Del Rossi G, Horodyski M, Kaminski T.W. Management of cervical-spine injuries. Athl Ther Today. 2002;7(2):46–51.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
