

Mitigation measures for pandemic influenza in Italy: an individual based model considering different scenarios
- PMID: 18335060
- PMCID: PMC2258437
- DOI: 10.1371/journal.pone.0001790
Mitigation measures for pandemic influenza in Italy: an individual based model considering different scenarios
Abstract
Background: Individual-based models can provide the most reliable estimates of the spread of infectious diseases. In the present study, we evaluated the diffusion of pandemic influenza in Italy and the impact of various control measures, coupling a global SEIR model for importation of cases with an individual based model (IBM) describing the Italian epidemic.
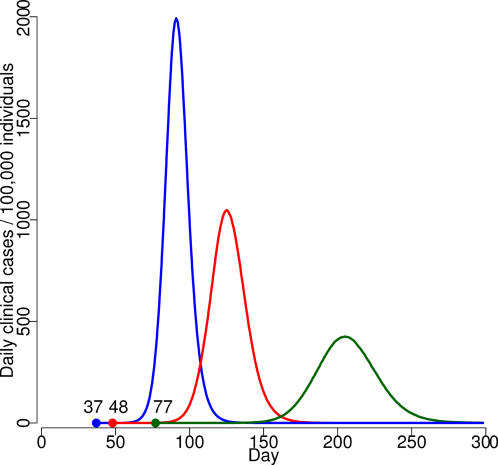
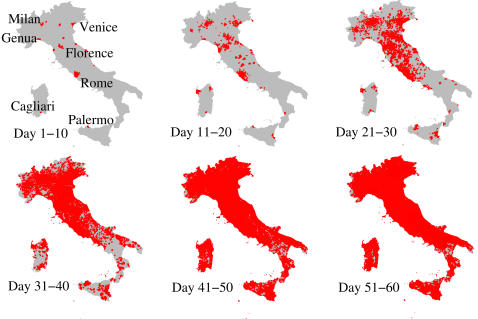
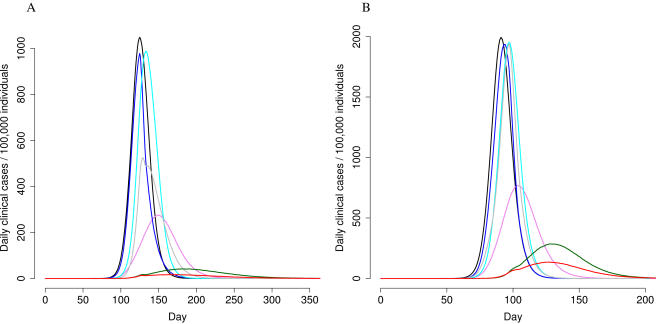
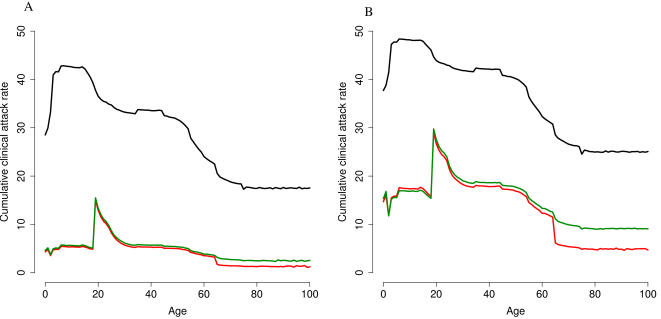
Methodology/principal findings: We co-located the Italian population (57 million inhabitants) to households, schools and workplaces and we assigned travel destinations to match the 2001 census data. We considered different R(0 )values (1.4; 1.7; 2), evaluating the impact of control measures (vaccination, antiviral prophylaxis -AVP-, international air travel restrictions and increased social distancing). The administration of two vaccine doses was considered, assuming that first dose would be administered 1-6 months after the first world case, and different values for vaccine effectiveness (VE). With no interventions, importation would occur 37-77 days after the first world case. Air travel restrictions would delay the importation of the pandemic by 7-37 days. With an R(0 )of 1.4 or 1.7, the use of combined measures would reduce clinical attack rates (AR) from 21-31% to 0.3-4%. Assuming an R(0) of 2, the AR would decrease from 38% to 8%, yet only if vaccination were started within 2 months of the first world case, in combination with a 90% reduction in international air traffic, closure of schools/workplaces for 4 weeks and AVP of household and school/work close contacts of clinical cases. Varying VE would not substantially affect the results.
Conclusions: This IBM, which is based on country-specific demographic data, could be suitable for the real-time evaluation of measures to be undertaken in the event of the emergence of a new pandemic influenza virus. All preventive measures considered should be implemented to mitigate the pandemic.
Conflict of interest statement
Figures
References
-
- Li KS, Guan Y, Wang J, Smith GJ, Xu KM, et al. Genesis of a highly pathogenic and potentially pandemic H5N1 influenza virus in eastern Asia. Nature. 2004;430:209–213. - PubMed
-
- World Health Organization. Epidemiology of WHO-confirmed human cases of avian influenza A(H5N1) infection. Wkly Epidemiol Rec. 2006;81:249–257. - PubMed
-
- World Health Organization. Outbreak news. Avian influenza, Turkey–update. Wkly Epidemiol Rec. 2006;81:42–43. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
