

Fracture risk in type 2 diabetes: update of a population-based study
- PMID: 18348689
- PMCID: PMC2574704
- DOI: 10.1359/jbmr.080323
Fracture risk in type 2 diabetes: update of a population-based study
Abstract
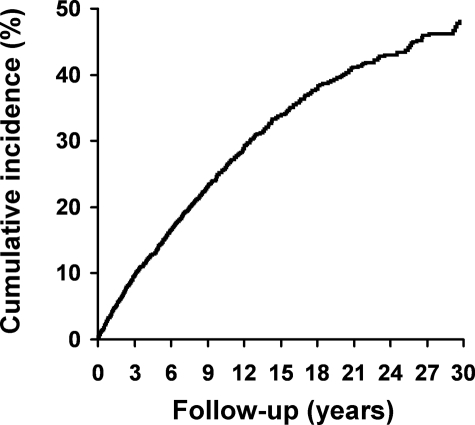
We found no significant excess of fractures among Rochester, MN, residents with diabetes mellitus initially recognized in 1950-1969, but more recent studies elsewhere have documented an apparent increase in hip fracture risk. To explore potential explanations for any increase in fractures, we performed an historical cohort study among 1964 Rochester residents who first met glycemic criteria for diabetes in 1970-1994 (mean age, 61.7 +/-14.0 yr; 51% men). Fracture risk was estimated by standardized incidence ratios (SIRs), and risk factors were evaluated in Andersen-Gill time-to-fracture regression models. In 23,236 person-years of follow-up, 700 diabetic residents experienced 1369 fractures documented by medical record review. Overall fracture risk was elevated (SIR, 1.3; 95% CI, 1.2-1.4), but hip fractures were increased only in follow-up beyond 10 yr (SIR, 1.5; 95% CI, 1.1-1.9). As expected, fracture risk factors included age, prior fracture, secondary osteoporosis, and corticosteroid use, whereas higher physical activity and body mass index were protective. Additionally, fractures were increased among patients with neuropathy (hazard ratio [HR], 1.3; 95% CI, 1.1-1.6) and those on insulin (HR, 1.3; 95% CI, 1.1-1.5); risk was reduced among users of biquanides (HR, 0.7; 95% CI, 0.6-0.96), and no significant influence on fracture risk was seen with sulfonylurea or thiazolidinedione use. Thus, contrary to our earlier study, the risk of fractures overall (and hip fractures specifically) was increased among Rochester residents with diabetes, but there was no evidence that the rise was caused by greater levels of obesity or newer treatments for diabetes.
Figures
References
-
- Heath H, III, Melton LJ, III, Chu CP. Diabetes mellitus and risk of skeletal fracture. N Engl J Med. 1980;303:567–570. - PubMed
-
- Daly PJ, Fitzgerald RH, Jr, Melton LJ, Ilstrup DM. Epidemiology of ankle fractures in Rochester, Minnesota. Acta Orthop Scand. 1987;58:539–544. - PubMed
-
- Seeley DG, Kelsey J, Jergas M, Nevitt MC. Predictors of ankle and foot fractures in older women. The Study of Osteoporotic Fractures Research Group. J Bone Miner Res. 1996;11:1347–1355. - PubMed
-
- Keegan TH, Kelsey JL, Sidney S, Quesenberry CP., Jr Foot problems as risk factors of fractures. Am J Epidemiol. 2002;155:926–931. - PubMed
-
- Hofbauer LC, Brueck CC, Singh SK, Dobnig H. Osteoporosis in patients with diabetes mellitus. J Bone Miner Res. 2007;22:1317–1328. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
