

Association of FKBP5 polymorphisms and childhood abuse with risk of posttraumatic stress disorder symptoms in adults
- PMID: 18349090
- PMCID: PMC2441757
- DOI: 10.1001/jama.299.11.1291
Association of FKBP5 polymorphisms and childhood abuse with risk of posttraumatic stress disorder symptoms in adults
Abstract
Context: In addition to trauma exposure, other factors contribute to risk for development of posttraumatic stress disorder (PTSD) in adulthood. Both genetic and environmental factors are contributory, with child abuse providing significant risk liability.
Objective: To increase understanding of genetic and environmental risk factors as well as their interaction in the development of PTSD by gene x environment interactions of child abuse, level of non-child abuse trauma exposure, and genetic polymorphisms at the stress-related gene FKBP5.
Design, setting, and participants: A cross-sectional study examining genetic and psychological risk factors in 900 nonpsychiatric clinic patients (762 included for all genotype studies) with significant levels of childhood abuse as well as non-child abuse trauma using a verbally presented survey combined with single-nucleotide polymorphism (SNP) genotyping. Participants were primarily urban, low-income, black (>95%) men and women seeking care in the general medical care and obstetrics-gynecology clinics of an urban public hospital in Atlanta, Georgia, between 2005 and 2007.
Main outcome measures: Severity of adult PTSD symptomatology, measured with the modified PTSD Symptom Scale, non-child abuse (primarily adult) trauma exposure and child abuse measured using the traumatic events inventory and 8 SNPs spanning the FKBP5 locus.
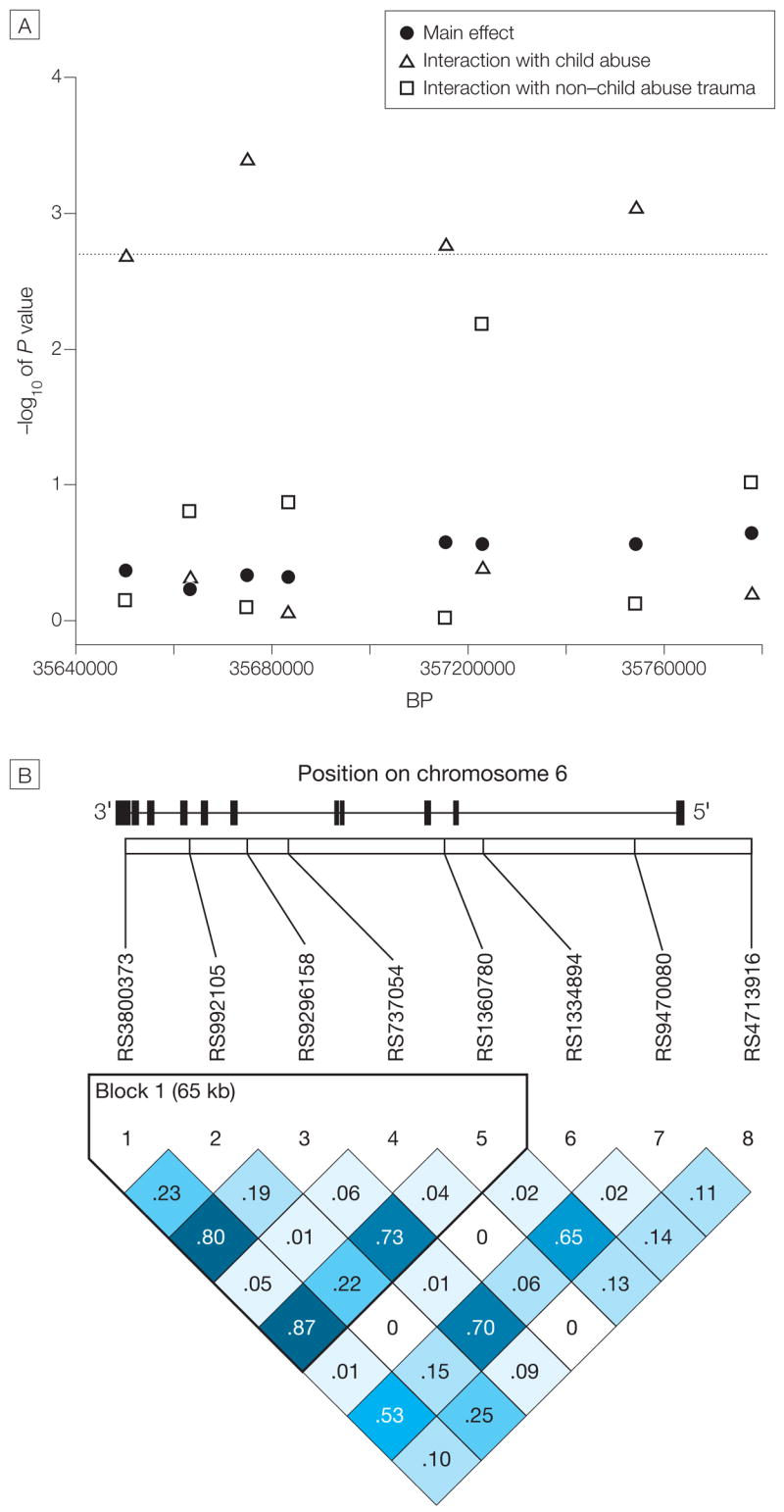
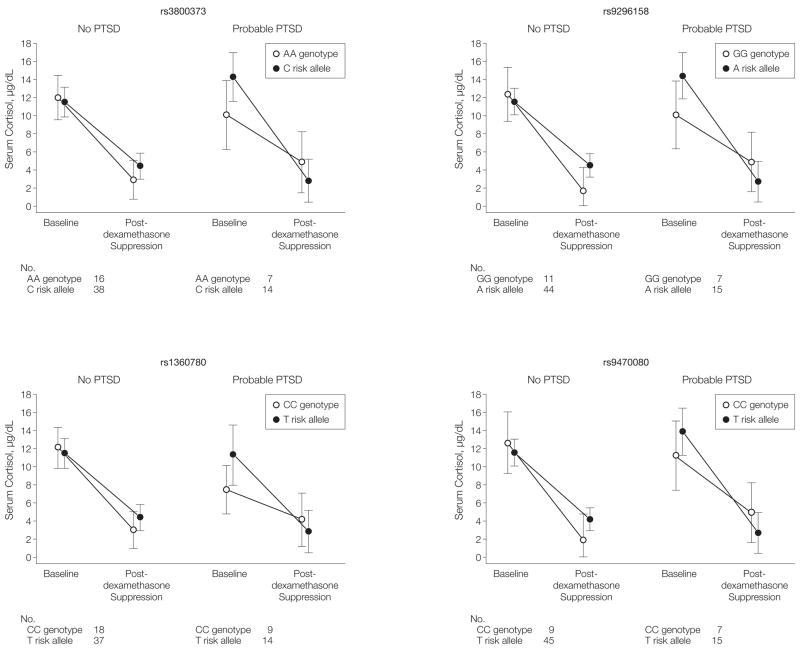
Results: Level of child abuse and non-child abuse trauma each separately predicted level of adult PTSD symptomatology (mean [SD], PTSD Symptom Scale for no child abuse, 8.03 [10.48] vs > or =2 types of abuse, 20.93 [14.32]; and for no non-child abuse trauma, 3.58 [6.27] vs > or =4 types, 16.74 [12.90]; P < .001). Although FKBP5 SNPs did not directly predict PTSD symptom outcome or interact with level of non-child abuse trauma to predict PTSD symptom severity, 4 SNPs in the FKBP5 locus significantly interacted (rs9296158, rs3800373, rs1360780, and rs9470080; minimum P = .0004) with the severity of child abuse to predict level of adult PTSD symptoms after correcting for multiple testing. This gene x environment interaction remained significant when controlling for depression severity scores, age, sex, levels of non-child abuse trauma exposure, and genetic ancestry. This genetic interaction was also paralleled by FKBP5 genotype-dependent and PTSD-dependent effects on glucocorticoid receptor sensitivity, measured by the dexamethasone suppression test.
Conclusions: Four SNPs of the FKBP5 gene interacted with severity of child abuse as a predictor of adult PTSD symptoms. There were no main effects of the SNPs on PTSD symptoms and no significant genetic interactions with level of non-child abuse trauma as predictor of adult PTSD symptoms, suggesting a potential gene-childhood environment interaction for adult PTSD.
Figures
References
-
- Hoge CW, Castro CA, Messer SC, et al. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. N Engl J Med. 2004;351(1):13–22. - PubMed
-
- Keane TM, Marshall AD, Taft CT. Posttraumatic stress disorder: etiology, epidemiology, and treatment outcome. Annu Rev Clin Psychol. 2006;2:161–197. - PubMed
-
- Yehuda R, McFarlane AC. Conflict between current knowledge about posttraumatic stress disorder and its original conceptual basis. Am J Psychiatry. 1995;152(12):1705–1713. - PubMed
-
- Nemeroff CB, Bremner JD, Foa EB, et al. Posttraumatic stress disorder: a state-of-the-science review. J Psychiatr Res. 2006;40(1):1–21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R56 MH071537/MH/NIMH NIH HHS/United States
- M01 RR00039/RR/NCRR NIH HHS/United States
- R01 MH071537/MH/NIMH NIH HHS/United States
- DA015766/DA/NIDA NIH HHS/United States
- MH069884/MH/NIMH NIH HHS/United States
- MH-42088/MH/NIMH NIH HHS/United States
- R01 MH042088/MH/NIMH NIH HHS/United States
- K01 MH069884/MH/NIMH NIH HHS/United States
- MH-58922/MH/NIMH NIH HHS/United States
- P50 MH058922/MH/NIMH NIH HHS/United States
- M01 RR000039/RR/NCRR NIH HHS/United States
- K02 DA015766/DA/NIDA NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- MH071537/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
