

Population-wide emergence of antiviral resistance during pandemic influenza
- PMID: 18350174
- PMCID: PMC2266801
- DOI: 10.1371/journal.pone.0001839
Population-wide emergence of antiviral resistance during pandemic influenza
Abstract
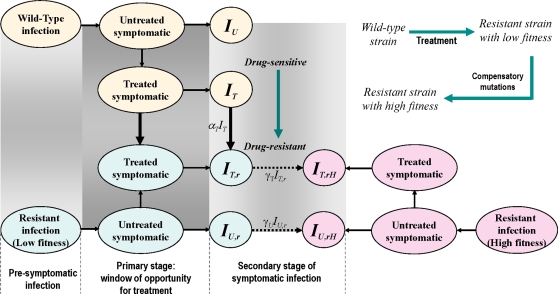
Background: The emergence of neuraminidase inhibitor resistance has raised concerns about the prudent use of antiviral drugs in response to the next influenza pandemic. While resistant strains may initially emerge with compromised viral fitness, mutations that largely compensate for this impaired fitness can arise. Understanding the extent to which these mutations affect the spread of disease in the population can have important implications for developing pandemic plans.
Methodology/principal findings: By employing a deterministic mathematical model, we investigate possible scenarios for the emergence of population-wide resistance in the presence of antiviral drugs. The results show that if the treatment level (the fraction of clinical infections which receives treatment) is maintained constant during the course of the outbreak, there is an optimal level that minimizes the final size of the pandemic. However, aggressive treatment above the optimal level can substantially promote the spread of highly transmissible resistant mutants and increase the total number of infections. We demonstrate that resistant outbreaks can occur more readily when the spread of disease is further delayed by applying other curtailing measures, even if treatment levels are kept modest. However, by changing treatment levels over the course of the pandemic, it is possible to reduce the final size of the pandemic below the minimum achieved at the optimal constant level. This reduction can occur with low treatment levels during the early stages of the pandemic, followed by a sharp increase in drug-use before the virus becomes widely spread.
Conclusions/significance: Our findings suggest that an adaptive antiviral strategy with conservative initial treatment levels, followed by a timely increase in the scale of drug-use, can minimize the final size of a pandemic while preventing large outbreaks of resistant infections.
Conflict of interest statement
Figures

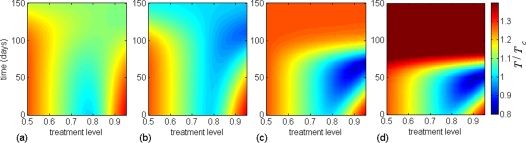
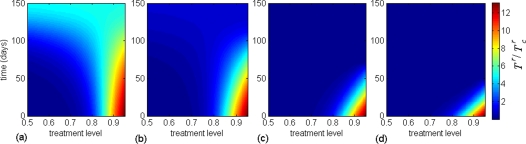
 ; (b)
; (b)  ; (c)
; (c)  ; and (d)
; and (d)  .
.
 (
( ,
,  ) and
) and  (
( ). Dashed curves in (a) and (b) correspond to the scenario in which no compensatory mutations occur, and resistant mutants are only present at low fitness cost.
). Dashed curves in (a) and (b) correspond to the scenario in which no compensatory mutations occur, and resistant mutants are only present at low fitness cost.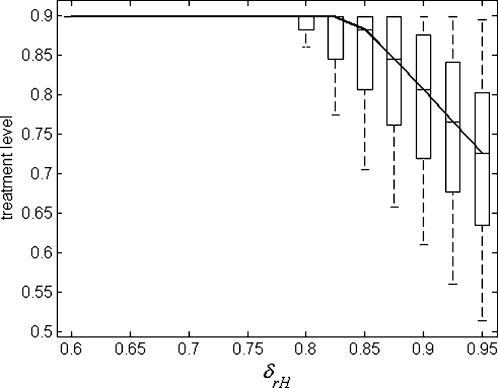

References
-
- Ferguson NM, Cummings DAT, Cauchemez S, Fraser C, Riley S, et al. Strategies for containing an emerging influenza pandemic in Southeast Asia. Nature. 2005;437:209–214. - PubMed
-
- Ferguson NM, Mallett S, Jackson H, Roberts N, Ward P. A population-dynamic model for evaluating the potential spread of drug-resistant influenza virus infections during community-based use of antivirals. J Antimicrob Chemother. 2003;51:977–990. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
