

Urine markers do not predict biopsy findings or presence of bladder ulcers in interstitial cystitis/painful bladder syndrome
- PMID: 18353383
- PMCID: PMC2705752
- DOI: 10.1016/j.juro.2008.01.047
Urine markers do not predict biopsy findings or presence of bladder ulcers in interstitial cystitis/painful bladder syndrome
Abstract
Purpose: We tested for associations between urine markers, bladder biopsy features and bladder ulcers in interstitial cystitis/painful bladder syndrome.
Materials and methods: Subjects were 72 patients with interstitial cystitis/painful bladder syndrome undergoing bladder distention and biopsy. Urine was collected before the procedure. Urine marker levels were correlated with biopsy and cystoscopic findings. Patients with no previous interstitial cystitis/painful bladder syndrome treatments (47) were analyzed separately from previously treated patients (25).
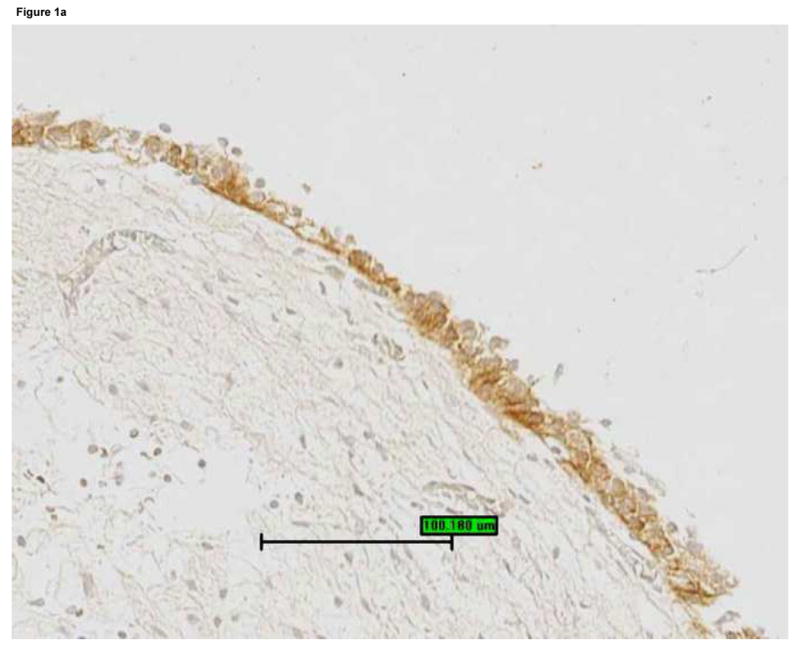
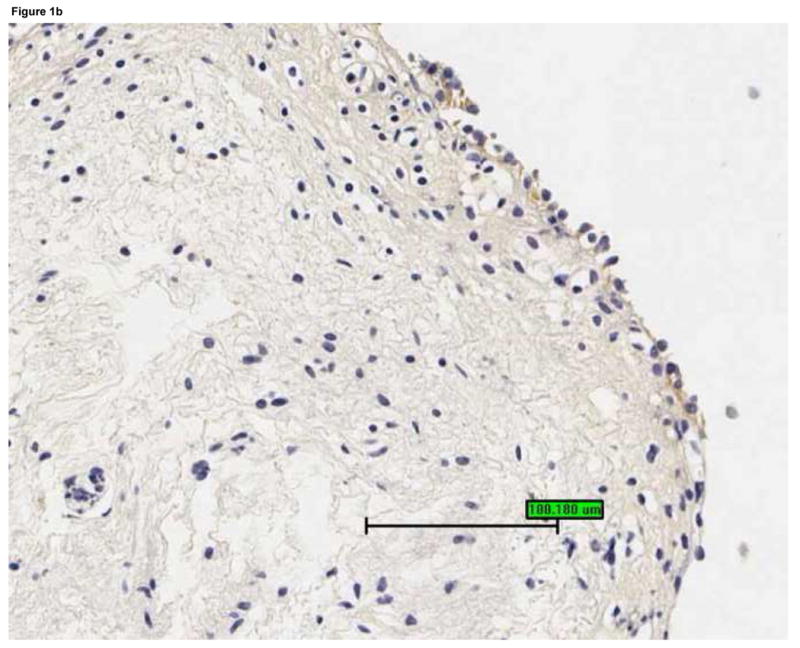
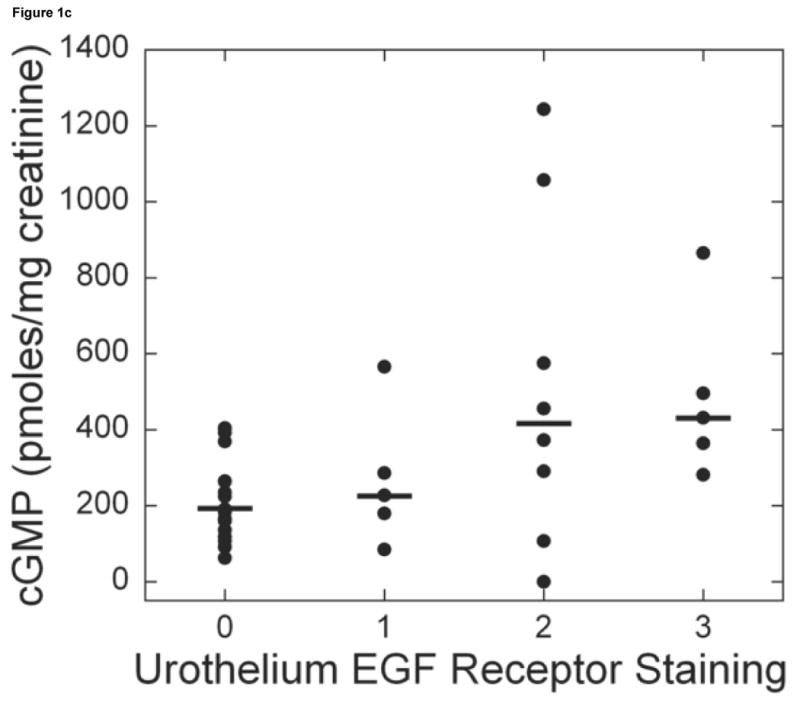
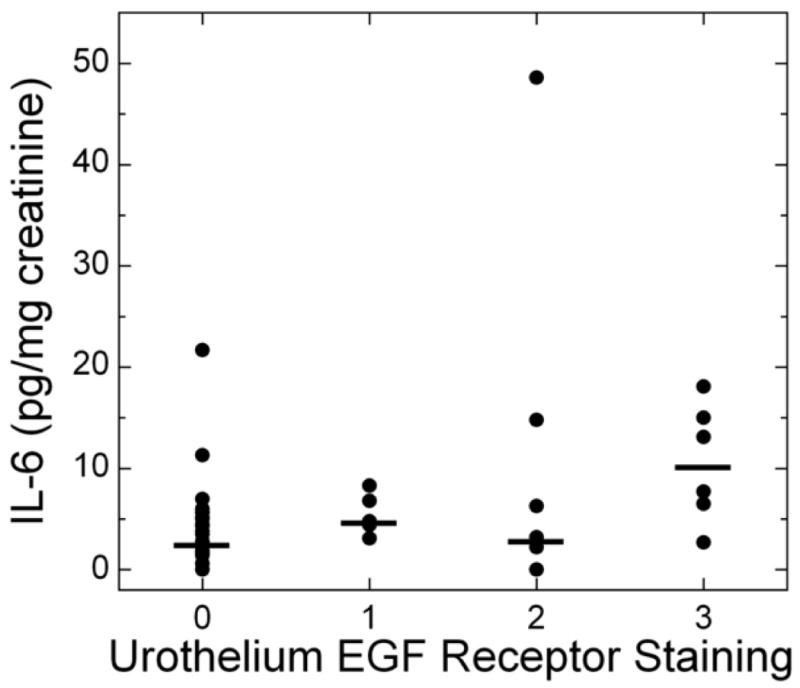
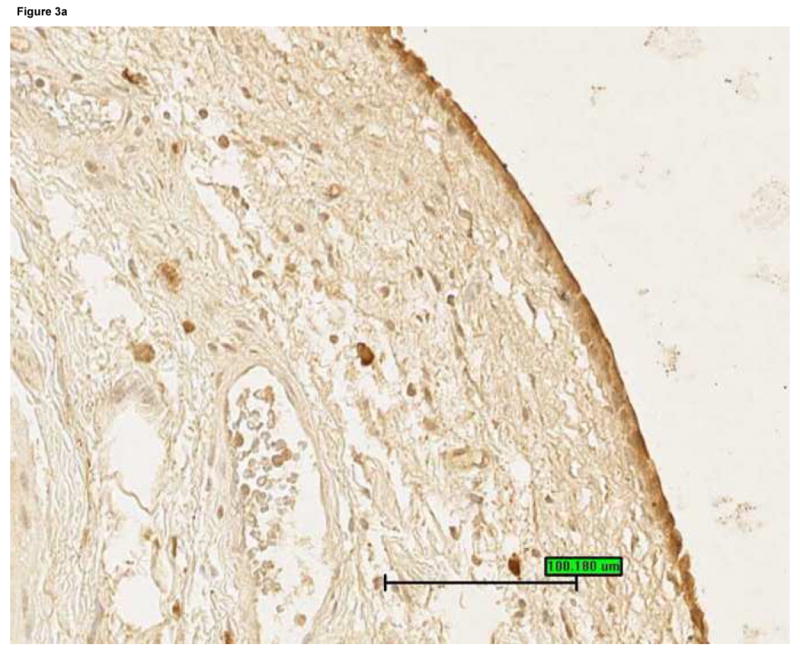
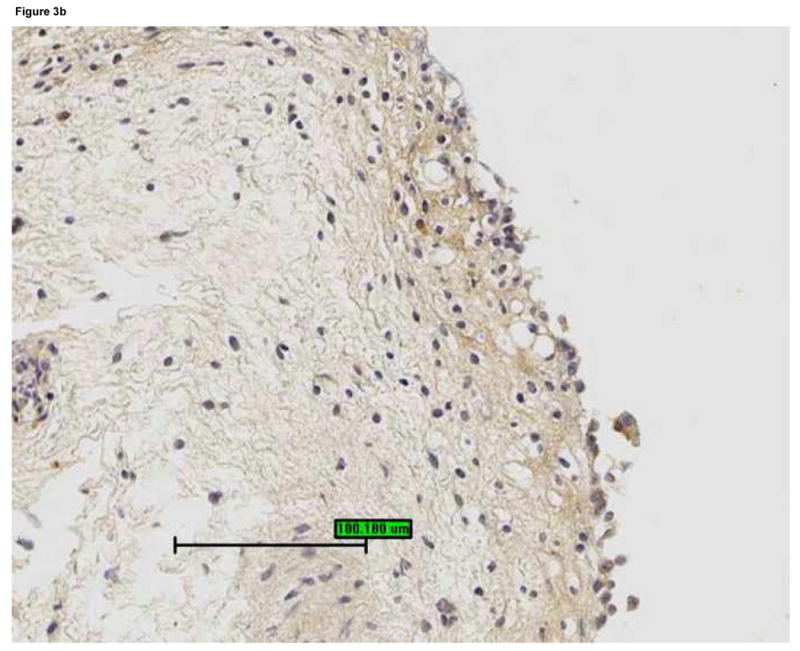
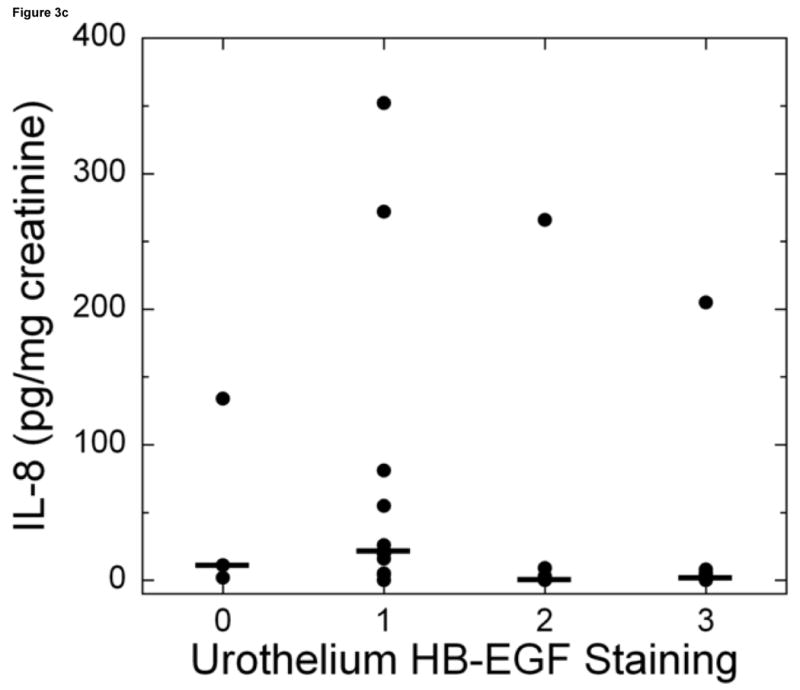
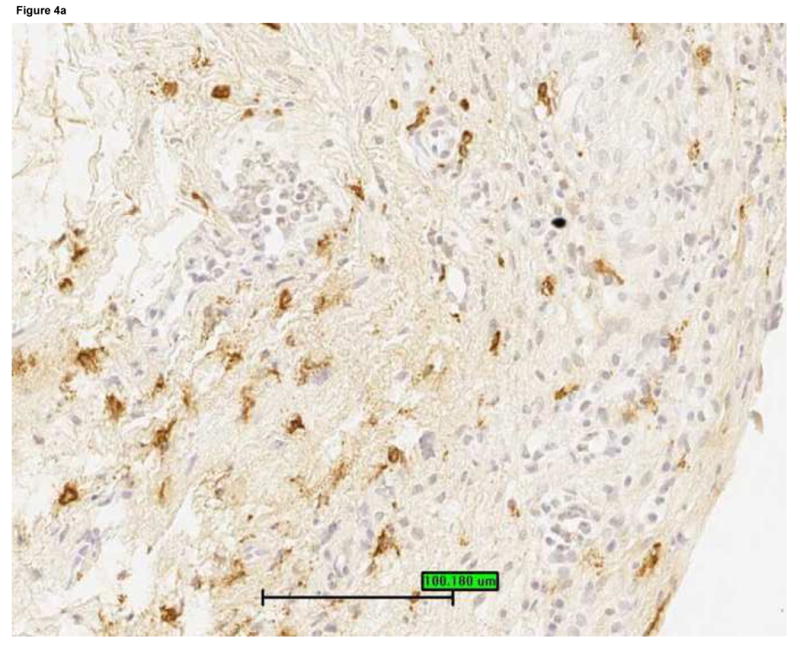
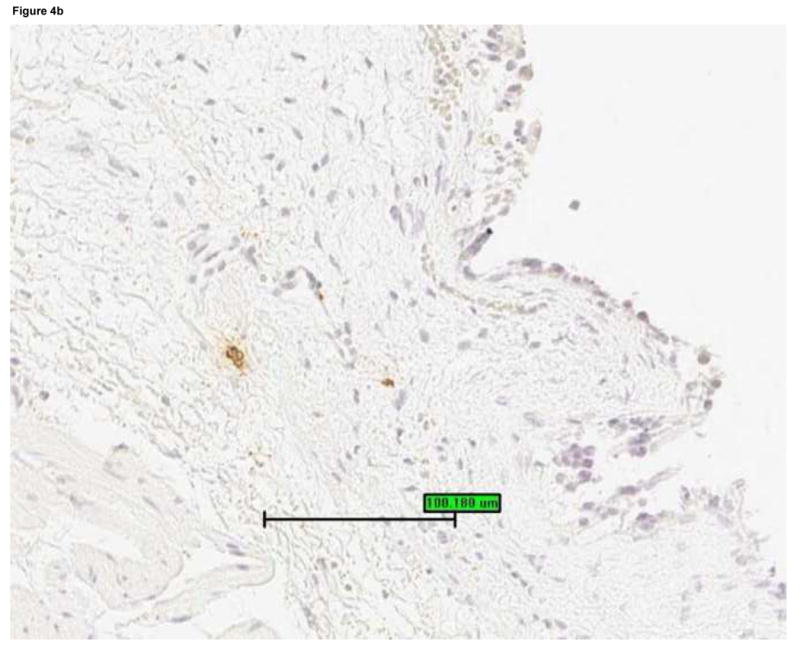
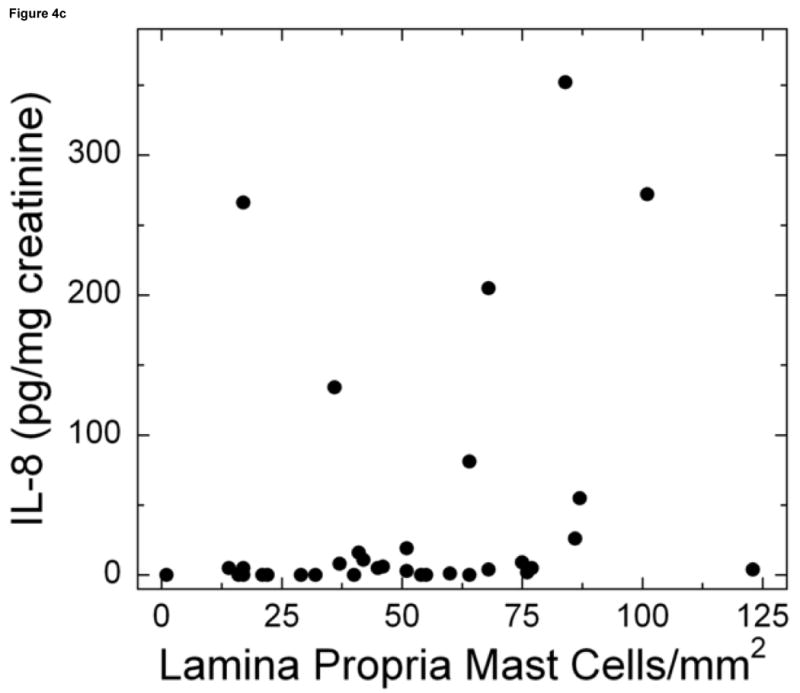
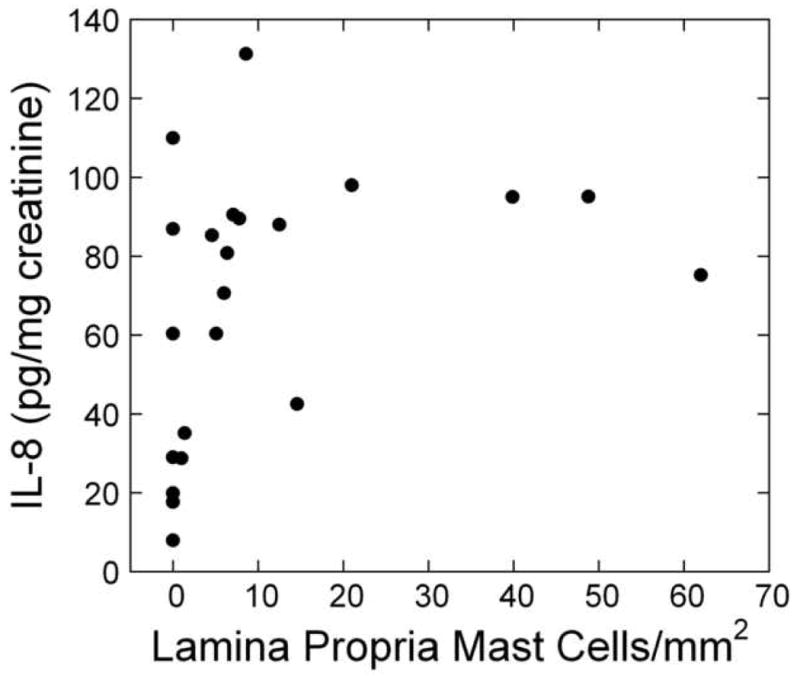
Results: For untreated patients urine interleukin-6 and cyclic guanosine monophosphate were associated with urothelial epidermal growth factor receptor staining (for interleukin-6 r = 0.29; 95% CI 0.07, 0.51; p = 0.01 and for cyclic guanosine monophosphate r = 0.34; 95% CI 0.13, 0.55; p = 0.002). Urine interleukin-8 was negatively associated with urothelial heparin-binding epidermal growth factor-like growth factor staining (r = -0.34; 95% CI -0.55, -0.12; p = 0.002) and positively associated with lamina propria mast cell count (r = 0.29; 95% CI 0.06, 0.52; p = 0.01). The latter association also was seen in treated patients (r = 0.46; 95% CI 0.20, 0.73; p <0.001). None of the urine markers was significantly different for ulcer vs nonulcer groups. All of the patients with ulcer had extensive inflammation on bladder biopsy including severe mononuclear cell infiltration, moderate or strong interleukin-6 staining in the urothelium and lamina propria, and leukocyte common antigen staining in more than 10% of the lamina propria. However, these features also were seen in 24% to 76% of the patients without ulcer.
Conclusions: Overall urine markers did not associate robustly with biopsy findings. The strongest association was a positive association between urine interleukin-8 levels and bladder mast cell count. Patients with ulcer consistently had bladder inflammation but the cystoscopic finding of ulcers was not a sensitive indicator of inflammation on bladder biopsy.
Figures
Comment in
-
A road map to biomarker discovery and validation in urological chronic pelvic pain syndrome.J Urol. 2008 May;179(5):1660-1. doi: 10.1016/j.juro.2008.02.010. Epub 2008 Mar 17. J Urol. 2008. PMID: 18343423 Free PMC article. No abstract available.
References
-
- Erickson DR, Tomaszewski JE, Kunselman AR, Bentley CM, Peters KM, Rovner ES, Demers LM, Wheeler MA, Keay SK. Do the National Institute of Diabetes and Digestive and Kidney Diseases cystoscopic criteria associate with other clinical and objective features of interstitial cystitis? J Urol. 2005;173:93. - PubMed
-
- Hanno PM, Landis JR, Matthews-Cook Y, Kusek J, Nyberg L the Interstitial Cystitis Database Study Group. The diagnosis of interstitial cystitis revisited: lessons learned from the National Institutes of Health Interstitial Cystitis Database Study. J Urol. 1999;161:553. - PubMed
-
- Erickson DR, Xie SX, Bhavanandan VP, Wheeler MA, Hurst RE, Demers LM, Kushner L, Keay SK. A comparison of multiple urine markers for interstitial cystitis. J Urol. 2002;167:2461. - PubMed
-
- Tomaszewski JE, Landis JR, Russack V, Williams TM, Wang LP, Hardy C, Brensinger C, Matthews YL, Abele ST, Kusek JW, Nyberg LM The Interstitial Cystitis Database Study Group. Biopsy features are associated with primary symptoms in interstitial cystitis: results from the interstitial cystitis database study. Urology. 2001;57(6 Suppl 1):67. - PubMed
-
- Peeker R, Fall M. Toward a precise definition of interstitial cystitis: further evidence of differences in classic and nonulcer disease. J Urol. 2002;167:2470. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
