

Monocyte chemoattractant protein-1 and macrophage inflammatory protein-1alpha as possible biomarkers for the chronic pelvic pain syndrome
- PMID: 18353390
- PMCID: PMC2786778
- DOI: 10.1016/j.juro.2008.01.028
Monocyte chemoattractant protein-1 and macrophage inflammatory protein-1alpha as possible biomarkers for the chronic pelvic pain syndrome
Abstract
Purpose: The chronic pelvic pain syndrome is characterized by pelvic pain, voiding symptoms and varying degrees of inflammation within expressed prostatic secretions. We evaluated the chemokines monocyte chemoattractant protein 1 (CCL2) and macrophage inflammatory protein-1alpha (CCL3) in expressed prostatic secretions to identify marker increases associated with inflammatory (IIIA) and noninflammatory (IIIB) chronic pelvic pain syndrome. In addition, chemokine levels were correlated with clinical pain as determined by the National Institutes of Health chronic prostatitis symptom index.
Materials and methods: Expressed prostatic secretions were collected by digital rectal examination, and evaluated by enzyme linked immunosorbent assays for monocyte chemoattractant protein 1 and macrophage inflammatory protein-1alpha in 154 patients including controls (13), those with benign prostatic hyperplasia (54), chronic pelvic pain syndrome IIIA (37) and IIIB (50). Monocyte chemoattractant protein 1 and macrophage inflammatory protein-1alpha levels were compared between IIIA, IIIB and the control subgroups, and correlated against the chronic prostatitis symptom index and pain subscore using a Spearman test.
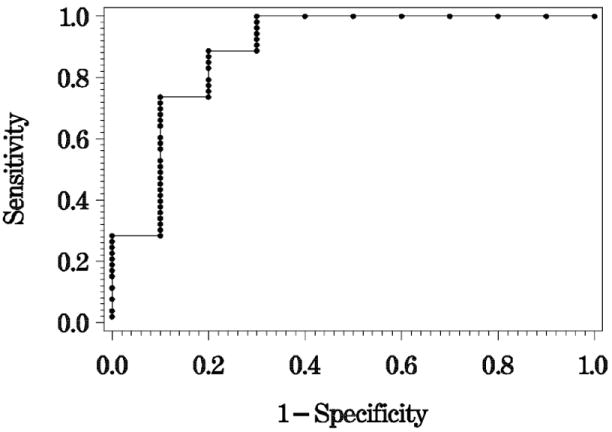
Results: Mean levels of monocyte chemoattractant protein 1 in the control, inflammatory benign prostatic hyperplasia, noninflammatory benign prostatic hyperplasia, inflammatory chronic pelvic pain syndrome and noninflammatory chronic pelvic pain syndrome were 599.4, 886.0, 1,636.5, 3,261.2 and 2,272.7 pg/ml, respectively. Mean levels of macrophage inflammatory protein-1alpha in the control, inflammatory benign prostatic hyperplasia, noninflammatory benign prostatic hyperplasia, IIIA chronic pelvic pain syndrome and IIIB chronic pelvic pain syndrome were 140.1, 299.4, 238.7, 1,057.8 and 978.4 pg/ml, respectively. For each cytokine both chronic pelvic pain syndrome subtypes had statistically higher levels than the control group and patients with benign prostatic hyperplasia (p = 0.0002). Receiver operating curves using monocyte chemoattractant protein 1 levels greater than 704 pg/ml and macrophage inflammatory protein-1alpha greater than 146 pg/ml identified patients with chronic pelvic pain syndrome with an accuracy of 90% from control patients. Macrophage inflammatory protein-1alpha levels (p = 0.0007) correlated with the pain subscore of the chronic prostatitis symptom index while monocyte chemoattractant protein 1 (p = 0.71) did not.
Conclusions: Monocyte chemoattractant protein 1 and macrophage inflammatory protein-1alpha within the prostatic fluid in both chronic pelvic pain syndrome subtypes provide candidate future biomarkers for chronic pelvic pain syndrome. In addition, macrophage inflammatory protein-1alpha increase in expressed prostatic secretions provides a new marker for clinical pain in chronic pelvic pain syndrome patients. Given these findings prostatic dysfunction likely has a role in the pathophysiology of this syndrome. These chemokines may serve as effective diagnostic markers and modulators against the chemokines could provide an attractive treatment strategy in individuals with chronic pelvic pain syndrome.
Figures


Comment in
-
A road map to biomarker discovery and validation in urological chronic pelvic pain syndrome.J Urol. 2008 May;179(5):1660-1. doi: 10.1016/j.juro.2008.02.010. Epub 2008 Mar 17. J Urol. 2008. PMID: 18343423 Free PMC article. No abstract available.
References
-
- Schaeffer AJ. Clinical practice. Chronic prostatitis and the chronic pelvic pain syndrome. N Engl J Med. 2006;355:1690. - PubMed
-
- Hochreiter WW, Nadler RB, Koch AE, Campbell PL, Ludwig M, Weidner W, et al. Evaluation of the cytokines interleukin 8 and epithelial neutrophil activating peptide 78 as indicators of inflammation in prostatic secretions. Urology. 2000;56:1025. - PubMed
-
- Nadler RB, Koch AE, Calhoun EA, Campbell PL, Pruden DL, Bennett CL, et al. IL-1beta and TNF-alpha in prostatic secretions are indicators in the evaluation of men with chronic prostatitis. J Urol. 2000;164:214. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
