

Empyema: an increasing concern in Canada
- PMID: 18354748
- PMCID: PMC2677840
- DOI: 10.1155/2008/975312
Empyema: an increasing concern in Canada
Abstract
Background: Empyema is a suppurative infection of the pleural space. Without prompt treatment, it can result in significant hospital stays, more invasive treatments as it progresses, and substantial morbidity and mortality.
Objectives: The primary objective of the present study was to evaluate whether there has been an increasing incidence of empyema in Canada. A secondary objective was to investigate whether this increase disproportionately affects any age group.
Methods: The Discharge Abstract Database of the Canadian Institute for Health Information was used to evaluate national empyema data.
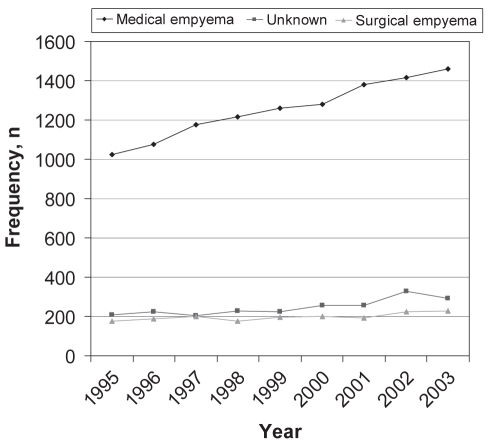
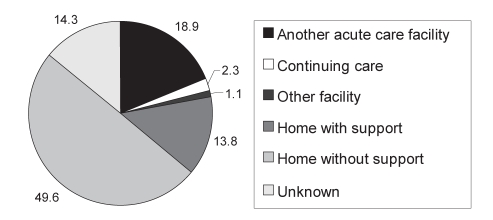
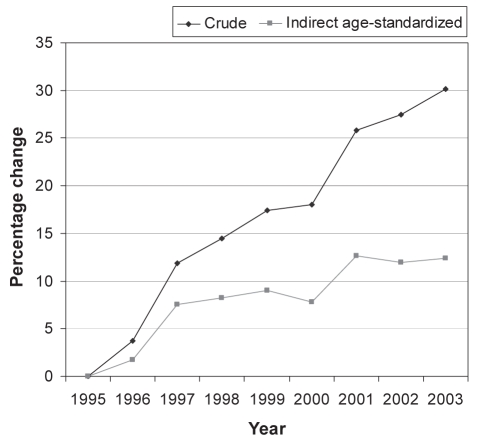
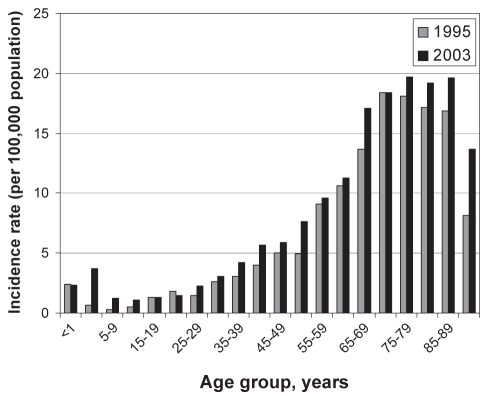
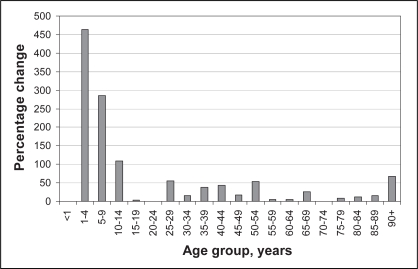
Results: There were 11,294 patients identified with empyema over the nine-year period of the present study, of whom 31% were women. The mean (+/- SD) length of stay was stable throughout the study at 21.82+/-33.88 days, and 63.4% were discharged home. The incidence rate ratio (IRR) was defined as the ratio of the incidence rate of medical empyema in 2003 divided by the incidence rate in 1995. Medical empyema increased significantly (IRR 1.30, 95% CI 1.20 to 1.41; P<0.001), as did empyema of unknown cause (IRR 1.29, 95% CI 1.08 to 1.54; P=0.005), while surgical empyema did not appear to increase (IRR 1.17, 95% CI 0.97 to 1.43; P=0.114). A Poisson regression showed an increase in the indirect age-standardized IRR during the study period (IRR 1.025, 95% CI 1.018 to 1.032; P<0.001). The IRR for patients younger than 19 years of age from 1995 to 2003 was 2.20 (95% CI 1.56 to 3.10), while the IRR in patients older than 19 years was 1.23 (95% CI 1.14 to 1.34).
Conclusions: The present study demonstrates the increasing rate of empyema in Canada and shows a change in pattern of disease. The disproportionate rate change in the pediatric population suggests a high-risk group that needs to be addressed. In the adult population, while cause is unknown, it is necessary to continually educate front-line physicians to confront both the increased burden of this disease, caused by an aging population, and the underlying increasing rate of empyema in Canada.
HISTORIQUE :: L’empyème est une infection suppurative de l’espace pleural. Sans une intervention rapide, il peut occasionner des taux d’hospitalisation importants, des traitements plus invasifs à mesure que la maladie progresse et une morbidité et mortalité substantielles.
OBJECTIFS :: Le principal objectif de la présente étude était de vérifier si l’empyème a augmenté au Canada. Le second objectif était de vérifier si ce problème affecte un groupe d’âge plus qu’un autre.
MÉTHODES :: Les auteurs ont interrogé la base de données sur les congés des patients de l’Institut canadien d’information sur la santé pour analyser les données sur l’empyème à l’échelon national.
RÉSULTATS :: L’empyème a été diagnostiqué chez 11 294 patients au cours de la période de neuf ans couverte par la présente étude; 31 % étaient des femmes. La durée moyenne (± É.-T.) du séjour est demeurée stable tout au long de l’étude soit 21,82 ± 33,88 jours et 63,4 % ont quitté pour retourner à la maison. Le taux d’incidence (TI) a été défini par l’incidence d’empyème médical en 2003, divisée par son incidence en 1995. L’empyème médical a significativement augmenté (TI 1,30, IC à 95 % 1,20 à 1,41, p < 0,001), tout comme l’empyème de cause inconnue (TI 1,29, IC à 95 % 1,08 à 1,54, p = 0,005), tandis que l’empyème chirurgical n’a pas semblé augmenter (TI 1,17, IC à 95 % 0,97 à 1,43, p = 0,114). Une analyse de régression de Poisson a révélé une augmentation du TI indirect standardisé selon l’âge durant la période de l’étude (TI 1,025, IC à 95 % 1,018 à 1,032, p < 0,001). Le TI chez les patients de moins de 19 ans entre 1995 et 2003 a été de 2,20 (IC à 95 % 1,56 à 3,10), tandis que chez les patients de plus de 19 ans il a été de 1,23 (IC à 95 % 1,14 à 1,34).
CONCLUSIONS :: La présente étude montre l’augmentation des taux d’empyème au Canada et une modification du mode de présentation de la maladie. Le taux disproportionné de changement dans la population pédiatrique donne à penser qu’il existe un groupe à risque élevé sur lequel il y a lieu de se pencher. Chez la population adulte, bien que la cause soit inconnue, il faut continuer de prodiguer un enseignement aux médecins de premiers recours pour mieux s’attaquer au fardeau croissant de cette maladie associée au vieillissement de la population et au taux de croissance sous-jacent de l’empyème au Canada.
Figures
Comment in
-
Empyema.Can Respir J. 2008 Mar;15(2):69-70. doi: 10.1155/2008/927191. Can Respir J. 2008. PMID: 18441619 Free PMC article. No abstract available.
-
Empyema: an increasing concern in Canada.Can Respir J. 2008 May-Jun;15(4):219. doi: 10.1155/2008/109374. Can Respir J. 2008. PMID: 18668720 Free PMC article. No abstract available.
References
-
- Andrews NC, Parker EF, Shaw RR, Wilson NJ, Webb WR. Management of nontuberculous empyema. Am Rev Respir Dis. 1962;85:935–6.
-
- Colice GL, Curtis A, Deslauriers J, et al. Medical and surgical treatment of parapneumonic effusions: An evidence-based guideline Chest 20001181158–71.(Erratum in 2001;119:319) - PubMed
-
- Bartlett JG, Gorbach SL, Thadepalli H, Finegold SM. Bacteriology of empyema. Lancet. 1974;1:338–40. - PubMed
-
- Ashbaugh DG. Empyema thoracis. Factors influencing morbidity and mortality. Chest. 1991;99:1162–5. - PubMed
-
- Ahmed RA, Marrie TJ, Huang JQ. Thoracic empyema in patients with community-acquired pneumonia. Am J Med. 2006;119:877–83. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
