

Liver, muscle, and adipose tissue insulin action is directly related to intrahepatic triglyceride content in obese subjects
- PMID: 18355813
- PMCID: PMC2629391
- DOI: 10.1053/j.gastro.2008.01.075
Liver, muscle, and adipose tissue insulin action is directly related to intrahepatic triglyceride content in obese subjects
Abstract
Background & aims: Nonalcoholic fatty liver disease is associated with insulin resistance and diabetes. The purpose of this study was to determine the relationship between intrahepatic triglyceride (IHTG) content and insulin action in liver (suppression of glucose production), skeletal muscle (stimulation of glucose uptake), and adipose tissue (suppression of lipolysis) in nondiabetic obese subjects.
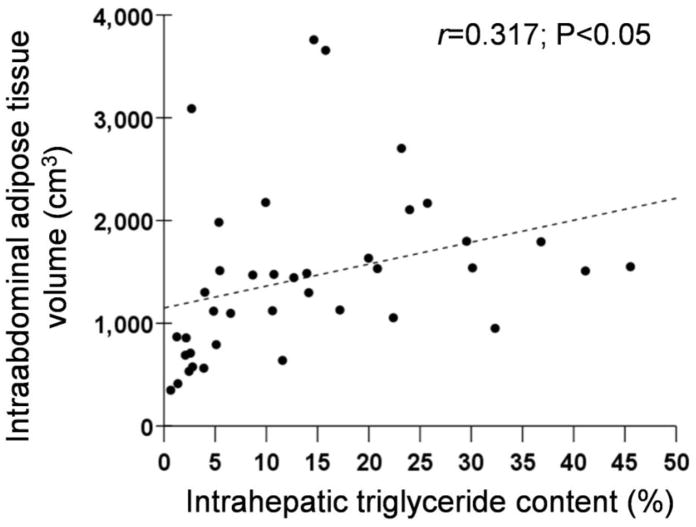
Methods: A euglycemic-hyperinsulinemic clamp procedure and stable isotopically labeled tracer infusions were used to assess insulin action, and magnetic resonance spectroscopy was used to determine IHTG content, in 42 nondiabetic obese subjects (body mass index, 36 +/- 4 kg/m(2)) who had a wide range of IHTG content (1%-46%).
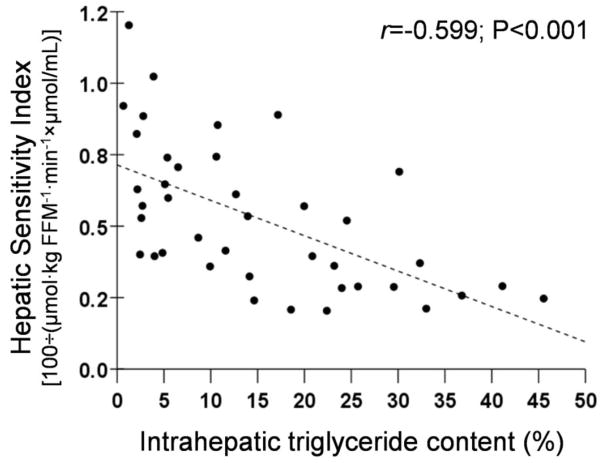
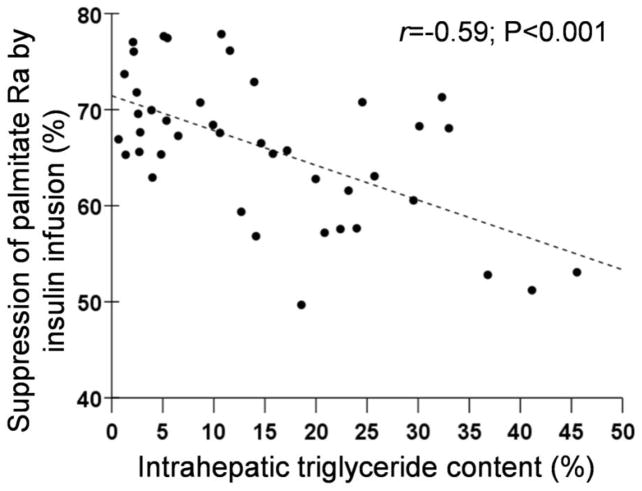
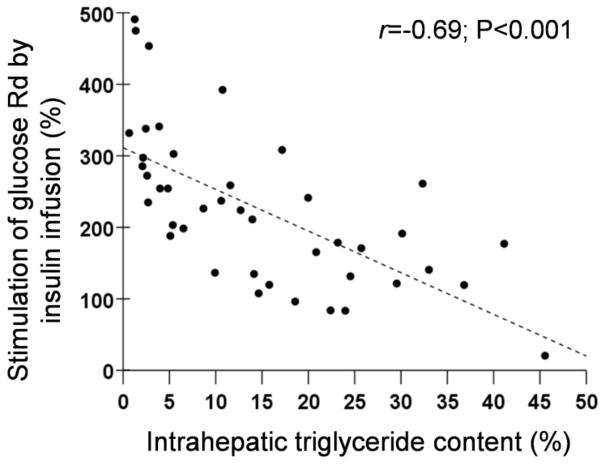
Results: Hepatic insulin sensitivity, assessed as a function of glucose production rate and plasma insulin concentration, was inversely correlated with IHTG content (r = -0.599; P < .001). The ability of insulin to suppress fatty acid release from adipose tissue and to stimulate glucose uptake by skeletal muscle were also inversely correlated with IHTG content (adipose tissue: r = -0.590, P < .001; skeletal muscle: r = -0.656, P < .001). Multivariate linear regression analyses found that IHTG content was the best predictor of insulin action in liver, skeletal muscle, and adipose tissue, independent of body mass index and percent body fat, and accounted for 34%, 42%, and 44% of the variability in these tissues, respectively (P < .001 for each model).
Conclusions: These results show that progressive increases in IHTG content are associated with progressive impairment of insulin action in liver, skeletal muscle, and adipose tissue in nondiabetic obese subjects. Therefore, nonalcoholic fatty liver disease should be considered part of a multiorgan system derangement in insulin sensitivity.
Figures
References
-
- Angulo P. Nonalcoholic fatty liver disease. N Engl J Med. 2002;346:1221–1231. - PubMed
-
- Marchesini G, Bugianesi E, Forlani G, Cerrelli F, Lenzi M, Manini R, Natale S, Vanni E, Villanova N, Melchionda N, Rizzetto M. Nonalcoholic fatty liver, steatohepatitis, and the metabolic syndrome. Hepatology. 2003;37:917–923. - PubMed
-
- Ioannou GN, Weiss NS, Boyko EJ, Mozaffarian D, Lee SP. Elevated serum alanine aminotransferase activity and calculated risk of coronary heart disease in the United States. Hepatology. 2006;43:1145–1151. - PubMed
-
- Adams LA, Lymp JF, St Sauver J, Sanderson SO, Lindor KD, Feldstein A, Angulo P. The natural history of nonalcoholic fatty liver disease: a population-based cohort study. Gastroenterology. 2005;129:113–121. - PubMed
-
- Ruhl CE, Everhart JE. Determinants of the association of overweight with elevated serum alanine aminotransferase activity in the United States. Gastroenterology. 2003;124:71–79. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
