

The UK Standardisation of Breast Radiotherapy (START) Trial B of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial
- PMID: 18355913
- PMCID: PMC2277488
- DOI: 10.1016/S0140-6736(08)60348-7
The UK Standardisation of Breast Radiotherapy (START) Trial B of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial
Abstract
Background: The international standard radiotherapy schedule for early breast cancer delivers 50 Gy in 25 fractions of 2.0 Gy over 5 weeks, but there is a long history of non-standard regimens delivering a lower total dose using fewer, larger fractions (hypofractionation). We aimed to test the benefits of radiotherapy schedules using fraction sizes larger than 2.0 Gy in terms of local-regional tumour control, normal tissue responses, quality of life, and economic consequences in women prescribed post-operative radiotherapy.
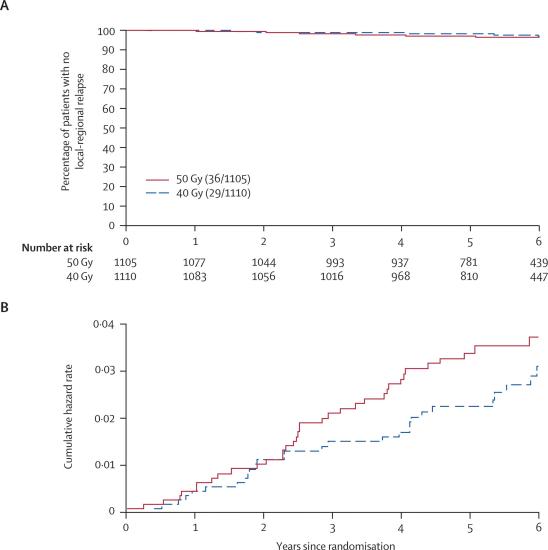
Methods: Between 1999 and 2001, 2215 women with early breast cancer (pT1-3a pN0-1 M0) at 23 centres in the UK were randomly assigned after primary surgery to receive 50 Gy in 25 fractions of 2.0 Gy over 5 weeks or 40 Gy in 15 fractions of 2.67 Gy over 3 weeks. Women were eligible for the trial if they were aged over 18 years, did not have an immediate reconstruction, and were available for follow-up. Randomisation method was computer generated and was not blinded. The protocol-specified principal endpoints were local-regional tumour relapse, defined as reappearance of cancer at irradiated sites, late normal tissue effects, and quality of life. Analysis was by intention to treat. This study is registered as an International Standard Randomised Controlled Trial, number ISRCTN59368779.
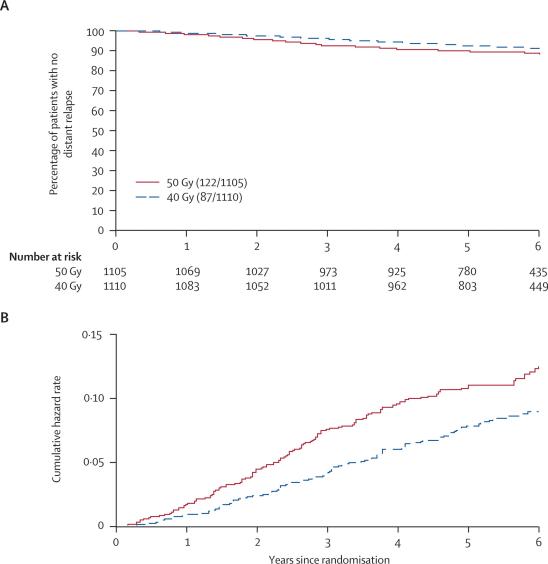
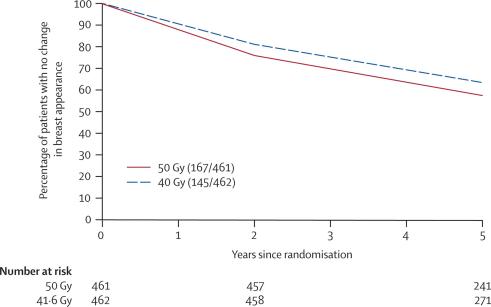
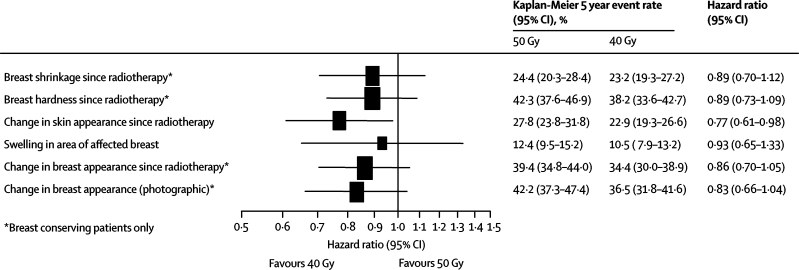
Findings: 1105 women were assigned to the 50 Gy group and 1110 to the 40 Gy group. After a median follow up of 6.0 years (IQR 5.0-6.2) the rate of local-regional tumour relapse at 5 years was 2.2% (95% CI 1.3-3.1) in the 40 Gy group and 3.3% (95% CI 2.2 to 4.5) in the 50 Gy group, representing an absolute difference of -0.7% (95% CI -1.7% to 0.9%)--ie, the absolute difference in local-regional relapse could be up to 1.7% better and at most 1% worse after 40 Gy than after 50 Gy. Photographic and patient self-assessments indicated lower rates of late adverse effects after 40 Gy than after 50 Gy.
Interpretation: A radiation schedule delivering 40 Gy in 15 fractions seems to offer rates of local-regional tumour relapse and late adverse effects at least as favourable as the standard schedule of 50 Gy in 25 fractions.
Figures

Comment in
-
Hypofractionation in radiotherapy for breast cancer.Lancet. 2008 Mar 29;371(9618):1050-2. doi: 10.1016/S0140-6736(08)60349-9. Epub 2008 Mar 19. Lancet. 2008. PMID: 18355914 No abstract available.
-
Radiotherapy hypofractionation in early breast cancer.Lancet. 2008 Jul 19;372(9634):203-4; author reply 205. doi: 10.1016/S0140-6736(08)61065-X. Lancet. 2008. PMID: 18640449 No abstract available.
-
Radiotherapy hypofractionation in early breast cancer.Lancet. 2008 Jul 19;372(9634):204; author reply 205. doi: 10.1016/S0140-6736(08)61066-1. Lancet. 2008. PMID: 18640451 No abstract available.
-
Radiotherapy hypofractionation in early breast cancer.Lancet. 2008 Jul 19;372(9634):204-5; author reply 205. doi: 10.1016/S0140-6736(08)61067-3. Lancet. 2008. PMID: 18640452 No abstract available.
References
-
- Fisher B, Redmond C, Fisher ER. Ten-year results of a randomized clinical trial comparing radical mastectomy and total mastectomy with or without radiation. N Engl J Med. 1985;312:674–681. - PubMed
-
- van Dongen JA, Bartelink H, Fentiman IS. Randomized clinical trial to assess the value of breast-conserving therapy in stage I and II breast cancer, EORTC 10801 trial. J Natl Cancer Inst Monogr. 1992;11:15–18. - PubMed
-
- Veronesi U, Luini A, Del Vecchio M. Radiotherapy after breast-preserving surgery in women with localized cancer of the breast. N Engl J Med. 1993;328:1587–1591. - PubMed
-
- Fisher B, Costantino J, Redmond C. Lumpectomy compared with lumpectomy and radiation therapy for the treatment of intraductal breast cancer. N Engl J Med. 1993;328:1581–1586. - PubMed
-
- Paterson R. The treatment of malignant disease by radium and x-rays. First edn. Edward Arnold; London: 1948.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
