

New insights into the pathogenesis of idiopathic hypercalciuria
- PMID: 18359393
- PMCID: PMC2362396
- DOI: 10.1016/j.semnephrol.2008.01.005
New insights into the pathogenesis of idiopathic hypercalciuria
Abstract
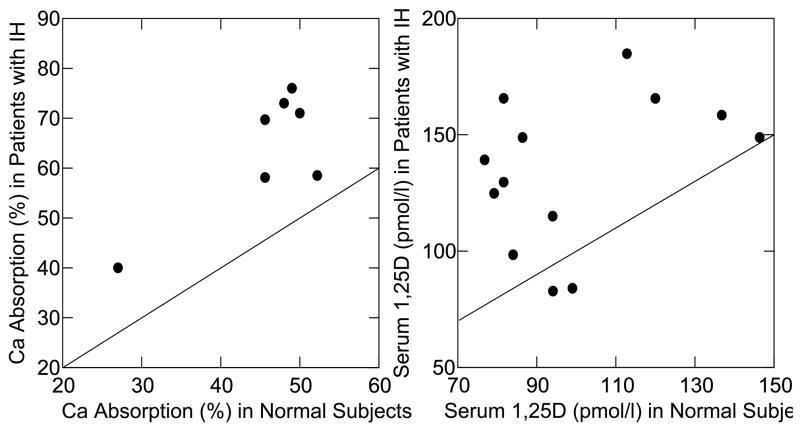
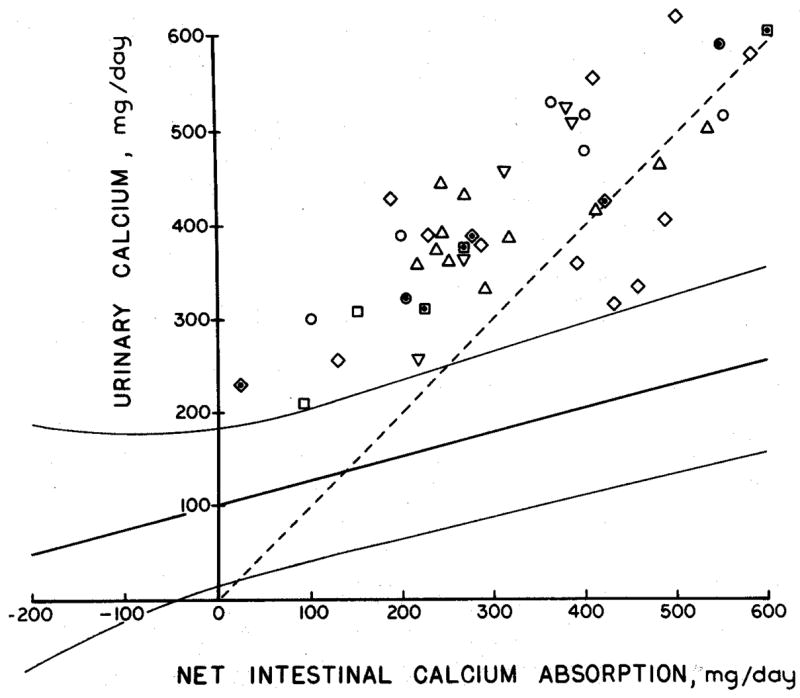
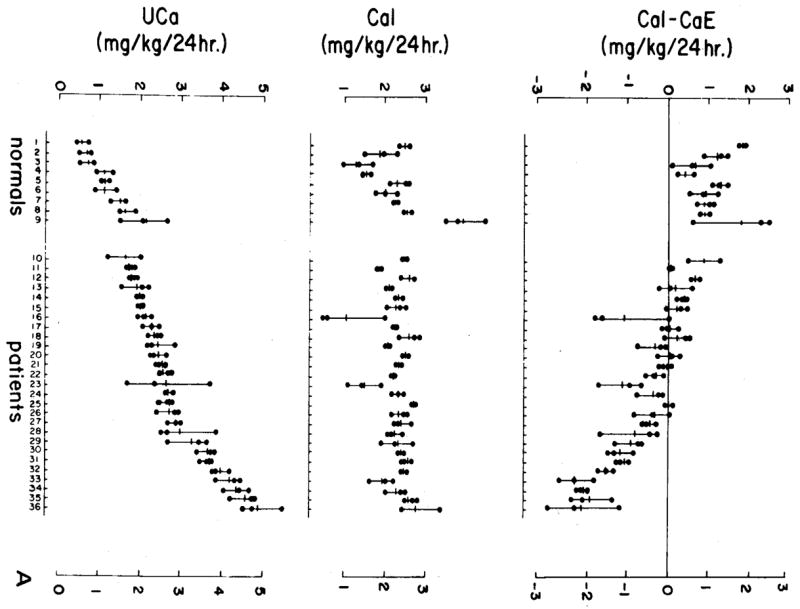
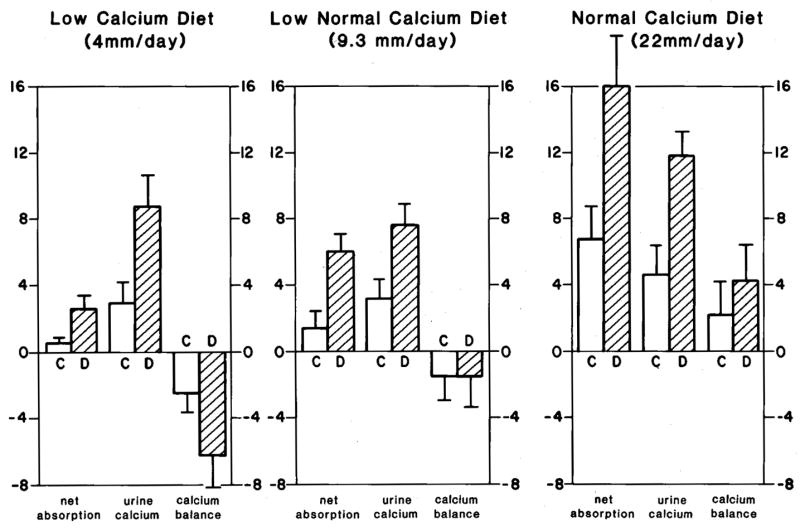
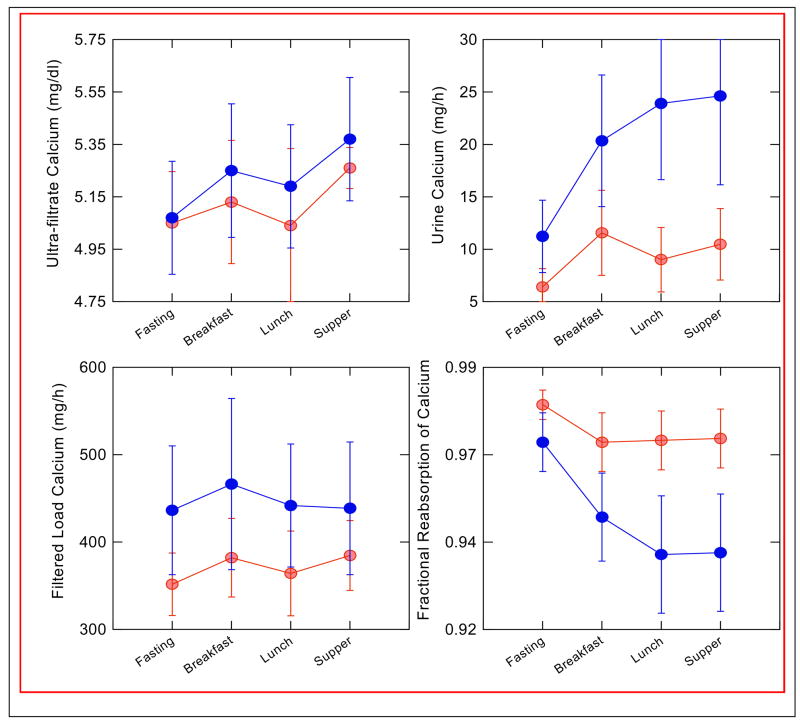
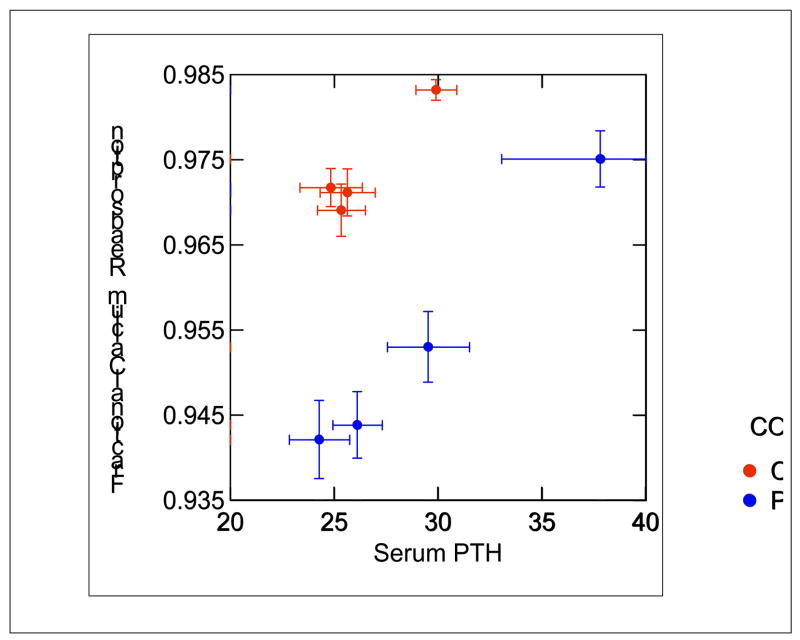
Idiopathic hypercalciuria (IH) is the most common metabolic abnormality in patients with calcium kidney stones. It is characterized by normocalcemia, absence of diseases that cause increased urine calcium, and calcium excretion that is greater than 250 mg/d in women and 300 mg/d in men. Subjects with IH have a generalized increase in calcium turnover, which includes increased gut calcium absorption, decreased renal calcium reabsorption, and a tendency to lose calcium from bone. Despite the increase in intestinal calcium absorption, a negative calcium balance is seen commonly in balance studies, especially on a low-calcium diet. The mediator of decreased renal calcium reabsorption is not clear; it is not associated with either an increase in filtered load of calcium or altered parathyroid hormone levels. There is an increased incidence of hypercalciuria in first-degree relatives of those with IH, but IH appears to be a complex polygenic trait with a large contribution from diet to expression of increased calcium excretion. Increased tissue vitamin D response may be responsible for the manifestations of IH in at least some patients.
Figures
References
-
- Hodkinson A, Pyrah LN. The urinary excretion of calcium and inorganic phosphate in 344 patients with calcium stone of renal origin. Br J Surg. 1958;48:10–18. - PubMed
-
- Coe FL. Treated and untreated recurrent calcium nephrolithiasis in patients with idiopathic hypercalciuria, hyperuricosuria, or no metabolic disorder. Ann Intern Med. 1977;87:404–410. - PubMed
-
- Flocks RH. Calcium and phosphorus excretion in the urine of patients with renal or ureteral calculi. JAMA. 1939;113:1466.
-
- Henneman PH, Benedict PH, Forbes AP, Dudley HR. Idiopathic Hypercalciuria. N Engl J Med. 1958;259:802–807. - PubMed
-
- van’t Hoff WG. Aetiological factors in paediatric urolithiasis. Nephron Clin Pract. 2004;98:45–48. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
