

Sputum analysis in diagnosis and management of obstructive airway diseases
- PMID: 18360557
- PMCID: PMC1661627
Sputum analysis in diagnosis and management of obstructive airway diseases
Abstract
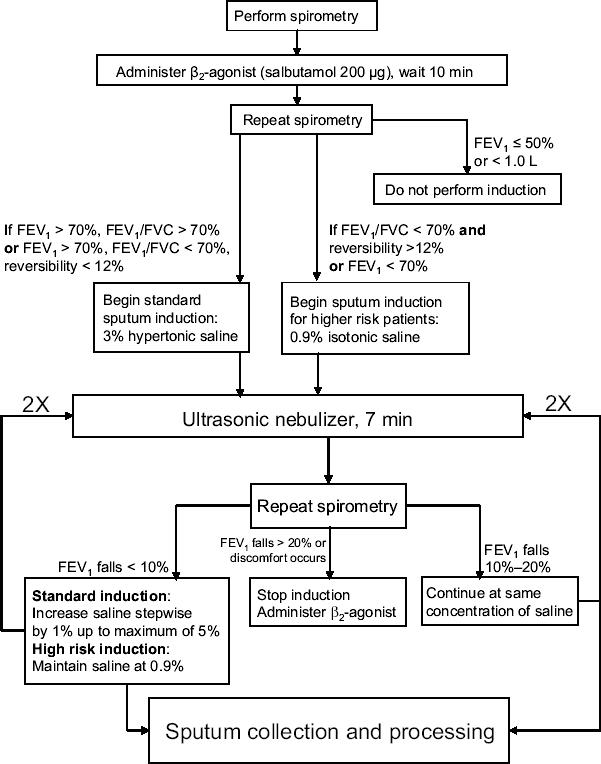
Induced sputum analysis has recently emerged as a potential new clinical tool in the diagnosis and management of obstructive airway diseases such as asthma, chronic obstructive pulmonary disease, and other disorders including bronchiectasis. Its safety has been demonstrated in numerous studies, and its efficacy is superior to previous techniques for determining airway inflammation. It is a noninvasive and highly reproducible approach in generating a measurable index of inflammatory cells in the airways of the lungs. Recent studies have shown that exacerbations, particularly in patients with moderate to severe asthma, can be reduced by routine analysis of induced sputum samples. We now have the ability to clinically apply sputum measurements to manage asthmatics. Inflammatory markers and cell types in induced sputum can also be investigated using newer technologies with more sensitive qualitative and quantitative features than basic cellular analysis. This review outlines the procedure for sputum induction, characterizes inflammatory cell types in the sputum, and addresses recent advances in the field of sputum analysis.
Figures
Similar articles
-
Determination of the inflammatory component of airway diseases by induced sputum cell counts: use in clinical practice.J Bras Pneumol. 2008 Nov;34(11):913-21. doi: 10.1590/s1806-37132008001100005. J Bras Pneumol. 2008. PMID: 19099097 English, Portuguese.
-
[Clinical application of induced and spontaneous sputum in asthma and chronic obstructive pulmonary disease].Orv Hetil. 2012 Nov 25;153(47):1847-54. doi: 10.1556/OH.2012.29494. Orv Hetil. 2012. PMID: 23160075 Review. Hungarian.
-
Sputum IL-25, IL-33 and TSLP, IL-23 and IL-36 in airway obstructive diseases. Reduced levels of IL-36 in eosinophilic phenotype.Cytokine. 2021 Apr;140:155421. doi: 10.1016/j.cyto.2021.155421. Epub 2021 Jan 22. Cytokine. 2021. PMID: 33486314
-
Heterogeneity of bronchitis in airway diseases in tertiary care clinical practice.Can Respir J. 2011 May-Jun;18(3):144-8. doi: 10.1155/2011/430317. Can Respir J. 2011. PMID: 21766077 Free PMC article.
-
Update on clinical inflammometry for the management of airway diseases.Can Respir J. 2013 Mar-Apr;20(2):117-20. doi: 10.1155/2013/602936. Can Respir J. 2013. PMID: 23616969 Free PMC article. Review.
Cited by
-
Comparing microbiota profiles in induced and spontaneous sputum samples in COPD patients.Respir Res. 2017 Aug 29;18(1):164. doi: 10.1186/s12931-017-0645-3. Respir Res. 2017. PMID: 28851370 Free PMC article.
-
A Novel Processing-Free Method for RNAseq Analysis of Spontaneous Sputum in Chronic Obstructive Pulmonary Disease.Front Pharmacol. 2021 Aug 19;12:704969. doi: 10.3389/fphar.2021.704969. eCollection 2021. Front Pharmacol. 2021. PMID: 34489698 Free PMC article.
-
Microbiology sampling in non-cystic fibrosis bronchiectasis cases from northern Alberta.PLoS One. 2023 Jul 14;18(7):e0288704. doi: 10.1371/journal.pone.0288704. eCollection 2023. PLoS One. 2023. PMID: 37450508 Free PMC article.
-
Oxidative Stress Markers in Sputum.Oxid Med Cell Longev. 2016;2016:2930434. doi: 10.1155/2016/2930434. Epub 2016 Jan 14. Oxid Med Cell Longev. 2016. PMID: 26885248 Free PMC article. Review.
-
Determining cystic fibrosis-affected lung microbiology: comparison of spontaneous and serially induced sputum samples by use of terminal restriction fragment length polymorphism profiling.J Clin Microbiol. 2010 Jan;48(1):78-86. doi: 10.1128/JCM.01324-09. Epub 2009 Nov 11. J Clin Microbiol. 2010. PMID: 19906901 Free PMC article.
References
-
- Adachi T, Motojima S, Hirata A, et al. Eosinophil viability-enhancing activity in sputum from patients with bronchial asthma. Contributions of interleukin-5 and granulocyte/macrophage colony-stimulating factor. Am J Respir Crit Care Med. 1995;151:618–23. - PubMed
-
- Anon Summary and recommendations of a workshop on the investigative use of fiberoptic bronchoscopy and bronchoalveolar lavage in asthmatics. Am Rev Respir Dis. 1985;132:180–2. - PubMed
-
- Asthma in America. 1998. Accessed 9 Mar 2005. URL: http://www.asthmainamerica.com
-
- Asthma in Canada. 2004. Accessed 9 Mar 2005. URL: http://www.asthmaincanada.com
-
- Barnes PJ. Chronic obstructive pulmonary disease. N Engl J Med. 2000;343:269–80. - PubMed
LinkOut - more resources
Full Text Sources