

Oxycodone controlled release in cancer pain management
- PMID: 18360598
- PMCID: PMC1936259
- DOI: 10.2147/tcrm.2006.2.3.229
Oxycodone controlled release in cancer pain management
Abstract
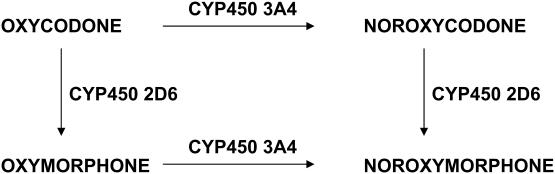
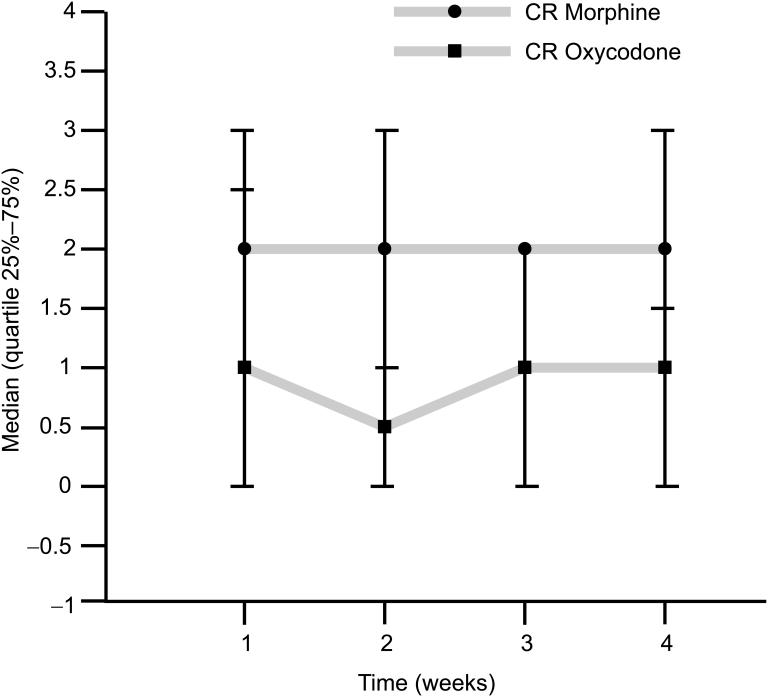
Oral opioids are the treatment of choice for chronic cancer pain. Morphine is the strong opioid of choice for the treatment of moderate to severe cancer pain according to guidelines from the World Health Organization (WHO). This recommendation by the WHO was derived from availability, familiarity to clinicians, established effectiveness, simplicity of administration, and relative inexpensive cost. It was not based on proven therapeutic superiority over other options. Patients who experience inadequate pain relief or intolerable side effects with one opioid may often be successfully treated with another agent or with the same agent administered by a different route. Opioid rotation, or switching to an alternative opioid, helps some patients achieve better pain control with fewer associated adverse effects. Oxycodone is a mu-opioid receptor specific ligand, with clear agonist properties. It is an active potent opioid, which is in part a kappa-receptor agonist. Like morphine and other pure agonists, there is no known ceiling to the analgesic effects of oxycodone. The active metabolites of oxycodone (eg, oxymorphone) could be important in oxycodone-mediated analgesia. The main pharmacokinetic difference between oxycodone and morphine is in oral bioavailability. The bioavailability of oxycodone is >60% and the bioavailability of morphine is 20%. Controlled-release oxycodone is absorbed in a bi-exponential fashion. There is a rapid phase with a mean half-life of 37 min, accounting for 38% of the dose, and a slow phase with a half-life of 6.2 h, which accounts for the residual 62%. Oxycodone elimination is impaired by renal failure because there are both an increased volume of distribution and reduced clearance. A lot of studies prove that the efficacy of controlled-release oxycodone in cancer-pain control is at least the same as morphine, immediate-release oxycodone and hydromorphone. Its toxicity profile seems better than that of morphine. There are actually several illustrations of a lower incidence of side-effects in the central nervous system. It is therefore possible to conclude that oxycodone represents a valid alternative to morphine in the management of moderate to severe cancer pain, also as first-line treatment.
Figures
References
-
- Beaver WT, Wallenstein SL, Rogers A, et al. Analgesic studies of codeine and oxycodone in patients with cancer. II. Comparisons of oral with intramuscular codeine and oral with intramuscular oxycodone. J Pharmacol Exp Ther. 1978a;207:101–8. - PubMed
-
- Beaver WT, Wallenstein SL, Rogers A, et al. Analgesic studies of codeine and oxycodone in patients with cancer. I. Comparisons of oral with intramuscular codeine and oral with intramuscular oxycodone. J Pharmacol Exp Ther. 1978b;207:92–100. - PubMed
-
- Bruera E, Belzile M, Pituskin E, et al. Randomized, double-blind, cross-over trial comparing safety and efficacy of oral controlled-release oxycodone with controlled-release morphine in patients with cancer pain. J Clin Oncol. 1998;16:3222–9. - PubMed
-
- Citron ML, Kaplan R, Parris WV, et al. Long-term administration of controlled-release oxycodone tablets for the treatment of cancer pain. Cancer Invest. 1998;16:562–71. - PubMed
-
- Davis MP, Varga J, Dickerson D, et al. Normal-release and controlled-release oxycodone: pharmacokinetcs, pharmacodynamics and controversy. Support Care Cancer. 2003;11:84–92. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
