

Optimal timing for antihypertensive dosing: focus on valsartan
- PMID: 18360620
- PMCID: PMC1936293
- DOI: 10.2147/tcrm.2007.3.1.119
Optimal timing for antihypertensive dosing: focus on valsartan
Abstract
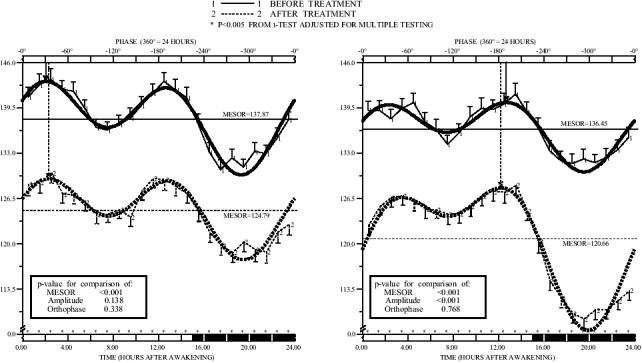
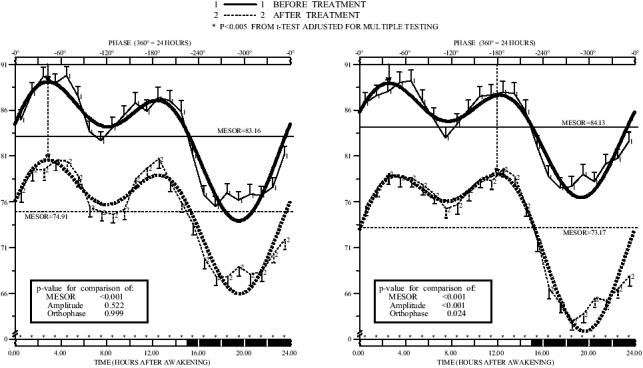
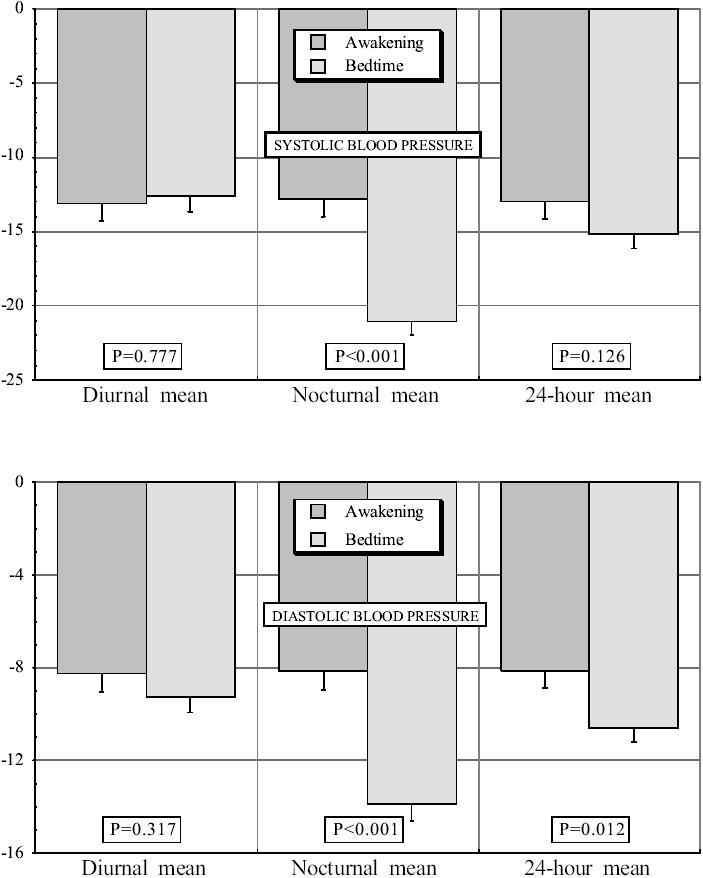
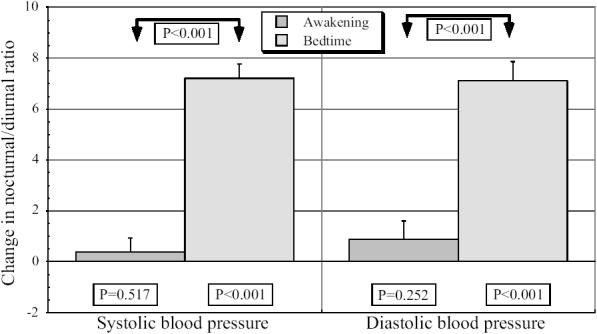
Some specific features of the 24 h blood pressure (BP) pattern are linked to the progressive injury of target tissues and the triggering of cardiac and cerebrovascular events. In particular, many studies show the extent of the nocturnal BP decline relative to the diurnal BP mean (the diurnal/nocturnal ratio, an index of BP dipping) is deterministic of cardiovascular injury and risk. Normalization of the circadian BP pattern is considered to be an important clinical goal of pharmacotherapy because it may slow the advance of renal injury and avert end-stage renal failure. The chronotherapy of hypertension takes into account the epidemiology of the BP pattern, plus potential administration-time determinants of the pharmacokinetics and dynamics of antihypertensive medications, as a means of enhancing beneficial outcomes and/or attenuating or averting adverse effects. Thus, bedtime dosing with nifedipine gastrointestinal therapeutic system (GITS) is more effective than morning dosing, while also reducing significantly secondary effects. The dose-response curve, therapeutic coverage, and efficacy of doxazosin GITS are all markedly dependent on the circadian time of drug administration. Moreover, valsartan administration at bedtime as opposed to upon wakening results in improved diurnal/nocturnal ratio, a significant increase in the percentage of patients with controlled BP after treatment, and significant reductions in urinary albumin excretion and plasma fibrinogen. Chronotherapy provides a means of individualizing treatment of hypertension according to the circadian BP profile of each patient, and constitutes a new option to optimize BP control and reduce risk.
Figures
References
-
- Anwar YA, Giacco S, McCabe EJ, et al. Evaluation of the efficacy of the Omron HEM-737 Intellisense device for use on adults according to the recommendations of the Association for the Advancement of Medical Instrumentation. Blood Press Monit. 1998;3:261–5. - PubMed
-
- Baumgart P. Circadian rhythm of blood pressure: Internal and external triggers. Chronobiol Int. 1991;8:444–50. - PubMed
-
- Bianchi S, Bigazzi R, Baldari G, et al. Diurnal variations of blood pressure and microalbuminuria in essential hypertension. Am J Hypertens. 1994;7:23–9. - PubMed
-
- Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. JAMA. 2003;289:2560–71. - PubMed
-
- Davis BR, Cutler JA, Furberg CD, et al. Relationship of antihypertensive treatment regimens and change in blood pressure to risk for heart failure in hypertensive patients randomly assigned to doxazosin or chlorthalidone: Further analyses from the antihypertensive and lipid-lowering treatment to prevent heart attack trial. Ann Intern Med. 2002;137(5 part 1):313–20. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
