

A computer modeling tool for comparing novel ICD electrode orientations in children and adults
- PMID: 18362024
- PMCID: PMC2745086
- DOI: 10.1016/j.hrthm.2008.01.018
A computer modeling tool for comparing novel ICD electrode orientations in children and adults
Abstract
Background: Use of implantable cardiac defibrillators (ICDs) in children and patients with congenital heart disease is complicated by body size and anatomy. A variety of creative implantation techniques has been used empirically in these groups on an ad hoc basis.
Objective: To rationalize ICD placement in special populations, we used subject-specific, image-based finite element models (FEMs) to compare electric fields and expected defibrillation thresholds (DFTs) using standard and novel electrode configurations.
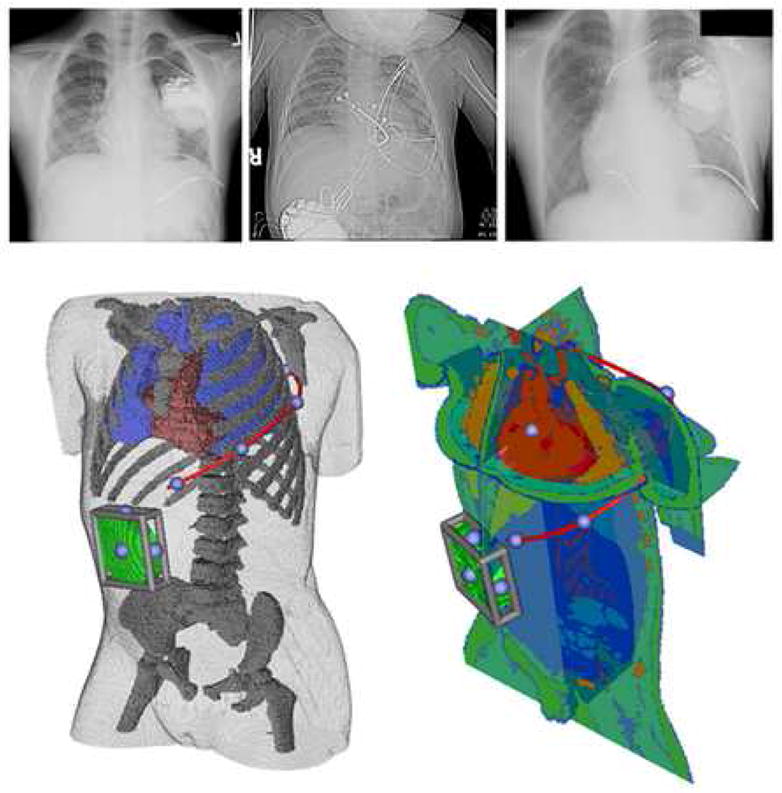
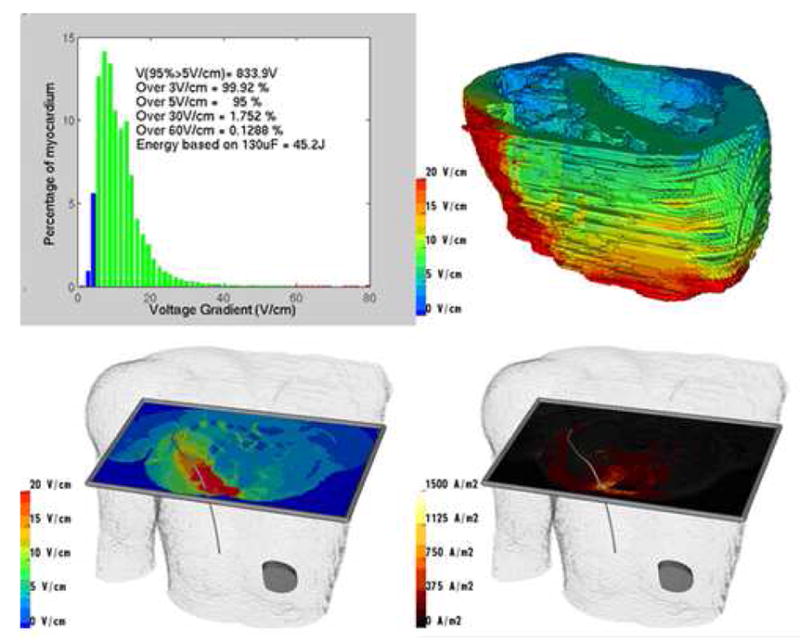
Methods: FEMs were created by segmenting normal torso computed tomography scans of subjects ages 2, 10, and 29 years and 1 adult with congenital heart disease into tissue compartments, meshing, and assigning tissue conductivities. The FEMs were modified by interactive placement of ICD electrode models in clinically relevant electrode configurations, and metrics of relative defibrillation safety and efficacy were calculated.
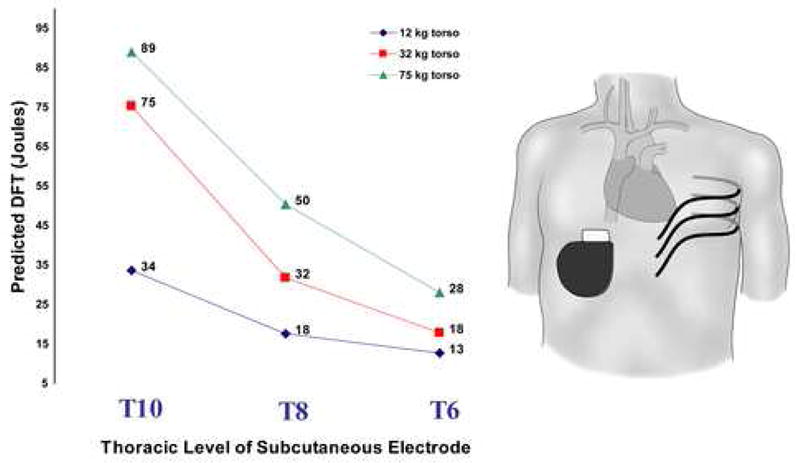
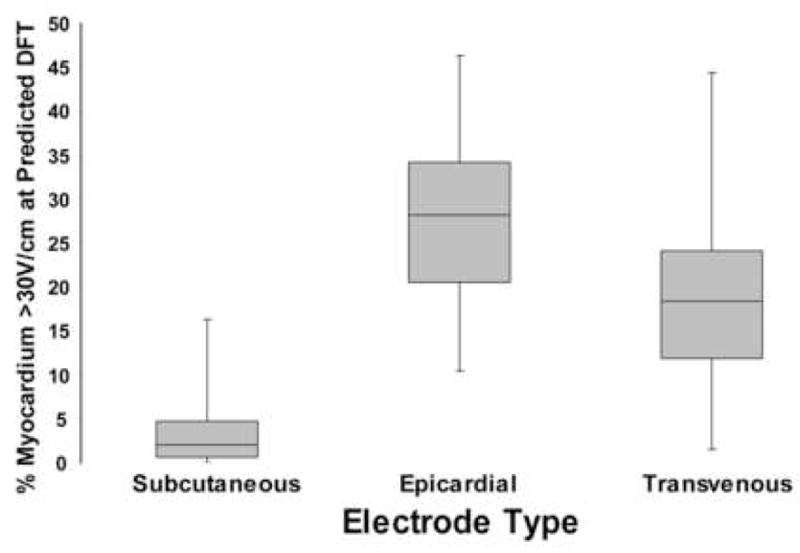
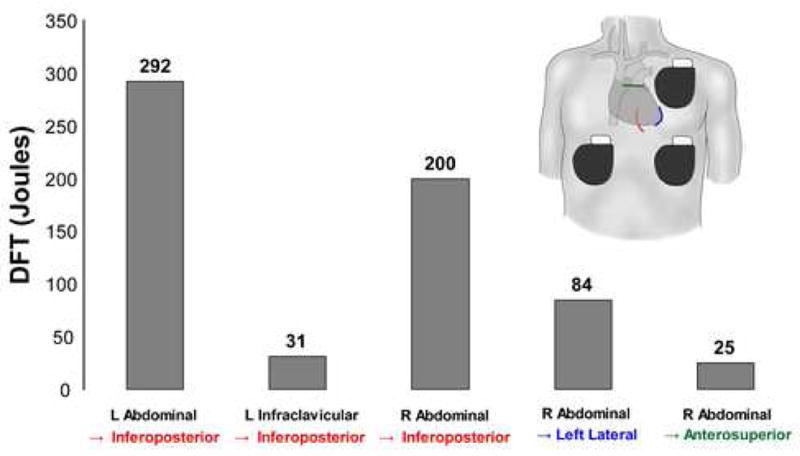
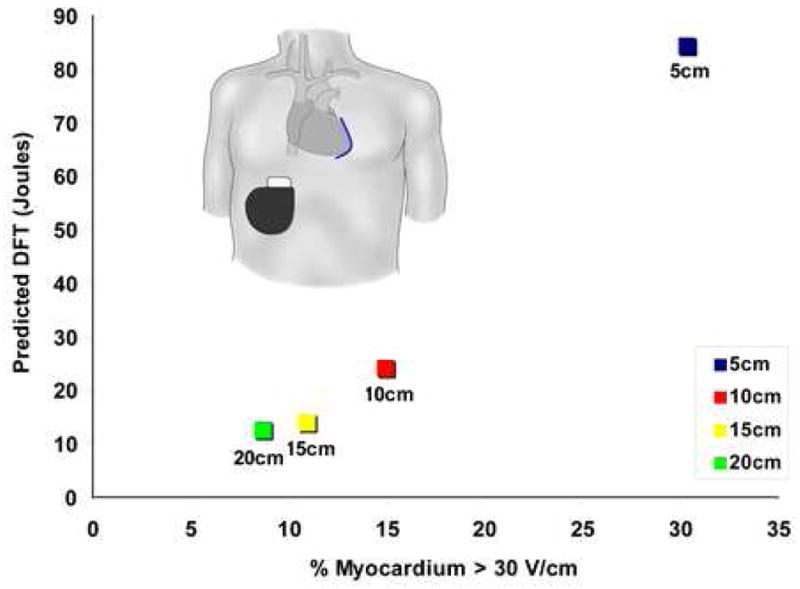
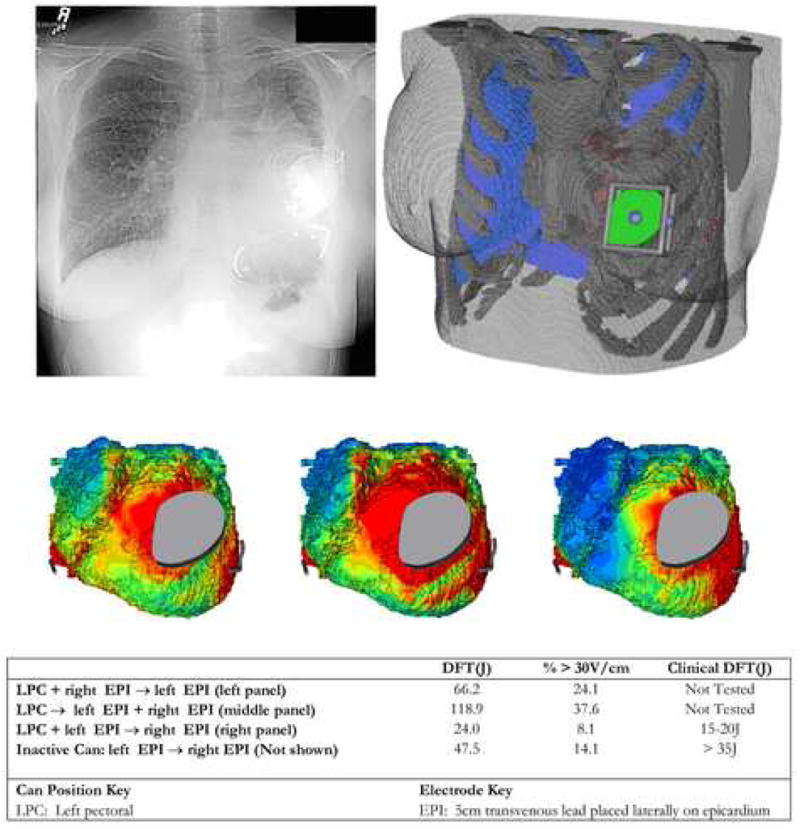
Results: Predicted DFTs for standard transvenous configurations were comparable with published results. Although transvenous systems generally predicted lower DFTs, a variety of extracardiac orientations were also predicted to be comparably effective in children and adults. Significant trend effects on DFTs were associated with body size and electrode length. In many situations, small alterations in electrode placement and patient anatomy resulted in significant variation of predicted DFT. We also show patient-specific use of this technique for optimization of electrode placement.
Conclusion: Image-based FEMs allow predictive modeling of defibrillation scenarios and predict large changes in DFTs with clinically relevant variations of electrode placement. Extracardiac ICDs are predicted to be effective in both children and adults. This approach may aid both ICD development and patient-specific optimization of electrode placement. Further development and validation are needed for clinical or industrial utilization.
Conflict of interest statement
There are no conflicts of interest to report
Figures
Comment in
-
Finite element modeling of novel ICD configurations in pediatric and congenital heart disease: validation of the MacGyver principle?Heart Rhythm. 2008 Apr;5(4):573-4. doi: 10.1016/j.hrthm.2008.02.040. Epub 2008 Mar 6. Heart Rhythm. 2008. PMID: 18362025 No abstract available.
Similar articles
-
Finite element modeling of subcutaneous implantable defibrillator electrodes in an adult torso.Heart Rhythm. 2010 May;7(5):692-8. doi: 10.1016/j.hrthm.2010.01.030. Epub 2010 Feb 1. Heart Rhythm. 2010. PMID: 20230927 Free PMC article.
-
Predictive modeling of defibrillation using hexahedral and tetrahedral finite element models: recent advances.J Electrocardiol. 2008 Nov-Dec;41(6):483-6. doi: 10.1016/j.jelectrocard.2008.08.002. Epub 2008 Sep 24. J Electrocardiol. 2008. PMID: 18817926 Free PMC article.
-
Generation of a cohort of whole-torso cardiac models for assessing the utility of a novel computed shock vector efficiency metric for ICD optimisation.Comput Biol Med. 2019 Sep;112:103368. doi: 10.1016/j.compbiomed.2019.103368. Epub 2019 Jul 24. Comput Biol Med. 2019. PMID: 31352217 Free PMC article.
-
[Transvenous subcutaneous implantation technique of the cardioverter/defibrillator].Herz. 1994 Oct;19(5):259-77. Herz. 1994. PMID: 8001899 Review. German.
-
Non-traditional implantable cardioverter-defibrillator configurations and insertion techniques: a review of contemporary options.Europace. 2022 Feb 2;24(2):181-192. doi: 10.1093/europace/euab178. Europace. 2022. PMID: 34453529 Free PMC article. Review.
Cited by
-
Computational Model for Therapy Optimization of Wearable Cardioverter Defibrillator: Shockable Rhythm Detection and Optimal Electrotherapy.Front Physiol. 2021 Dec 10;12:787180. doi: 10.3389/fphys.2021.787180. eCollection 2021. Front Physiol. 2021. PMID: 34955894 Free PMC article.
-
Finite element modeling of subcutaneous implantable defibrillator electrodes in an adult torso.Heart Rhythm. 2010 May;7(5):692-8. doi: 10.1016/j.hrthm.2010.01.030. Epub 2010 Feb 1. Heart Rhythm. 2010. PMID: 20230927 Free PMC article.
-
Temporal Dilation of Animal Cardiac Recordings Registered to Human Torso Geometries.Comput Cardiol (2010). 2016 Sep;43:329-332. Epub 2017 Mar 2. Comput Cardiol (2010). 2016. PMID: 28451593 Free PMC article.
-
Additional coils mitigate elevated defibrillation threshold in right-sided implantable cardioverter defibrillator generator placement: a simulation study.Europace. 2023 Jun 2;25(6):euad146. doi: 10.1093/europace/euad146. Europace. 2023. PMID: 37314196 Free PMC article.
-
Virtual electrodes around anatomical structures and their roles in defibrillation.PLoS One. 2017 Mar 2;12(3):e0173324. doi: 10.1371/journal.pone.0173324. eCollection 2017. PLoS One. 2017. PMID: 28253365 Free PMC article.
References
-
- Alexander ME, Cecchin F, Walsh EP, et al. Implications of implantable cardioverter defibrillator therapy in congenital heart disease and pediatrics. J Cardiovasc Electrophysiol. 2004;15:72–76. - PubMed
-
- Bokhari F, Newman D, Greene M, et al. Long-term comparison of the implantable cardioverter defibrillator versus amiodarone: eleven-year follow-up of a subset of patients in the Canadian Implantable Defibrillator Study (CIDS) Circulation. 2004;110:112–116. - PubMed
-
- Buxton AE, Lee KL, Fisher JD, et al. A randomized study of the prevention of sudden death in patients with coronary artery disease. New Engl J Med. 1999;341:1882–1890. - PubMed
-
- Moss AJ, Hall WJ, Cannom DS, et al. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. New Engl J Med. 1996;335:1933–1940. - PubMed
-
- Kugler JD, Erickson CC. Nontransvenous implantable cardioverter defibrillator systems: not just for small pediatric patients. J Cardiovasc Electrophysiol. 2006;17:47–48. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
