

Treatment success in cancer: new cancer treatment successes identified in phase 3 randomized controlled trials conducted by the National Cancer Institute-sponsored cooperative oncology groups, 1955 to 2006
- PMID: 18362256
- PMCID: PMC2773511
- DOI: 10.1001/archinte.168.6.632
Treatment success in cancer: new cancer treatment successes identified in phase 3 randomized controlled trials conducted by the National Cancer Institute-sponsored cooperative oncology groups, 1955 to 2006
Abstract
Background: The evaluation of research output, such as estimation of the proportion of treatment successes, is of ethical, scientific, and public importance but has rarely been evaluated systematically. We assessed how often experimental cancer treatments that undergo testing in randomized clinical trials (RCTs) result in discovery of successful new interventions.
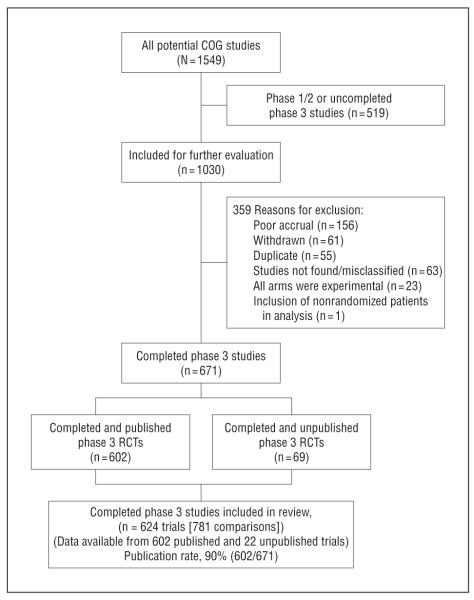
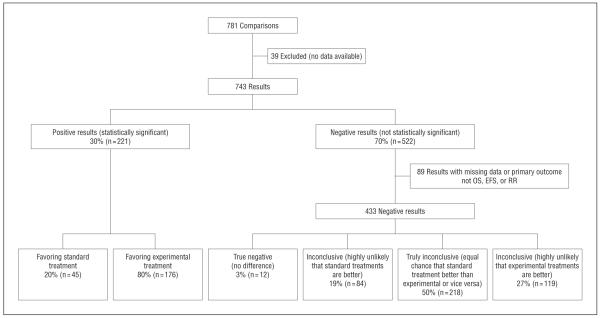
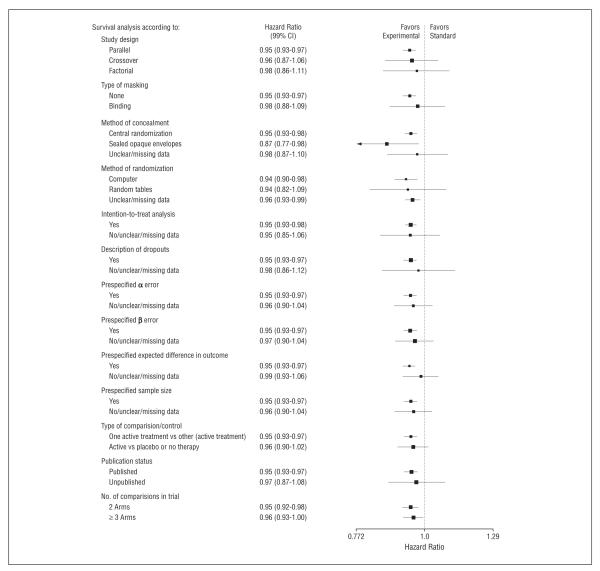
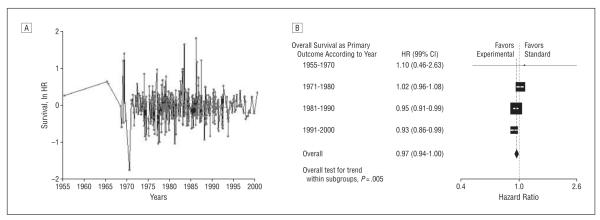
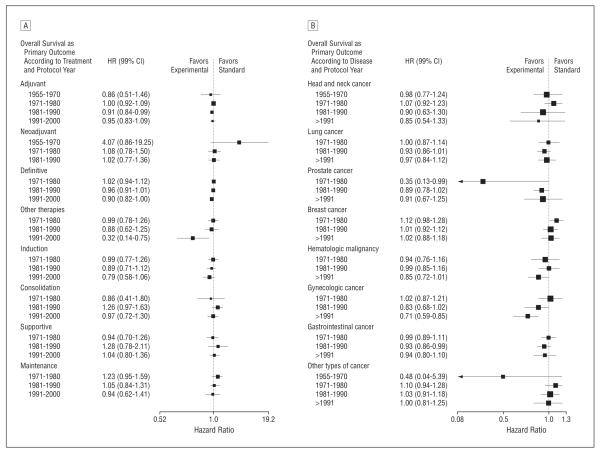
Methods: We extracted data from all completed (published and unpublished) phase 3 RCTs conducted by the National Cancer Institute cooperative groups since their inception in 1955. Therapeutic successes were determined by (1) assessing the proportion of statistically significant trials favoring new or standard treatments, (2) determining the proportion of the trials in which new treatments were considered superior to standard treatments according to the original researchers, and (3) quantitatively synthesizing data for main clinical outcomes (overall and event-free survival).
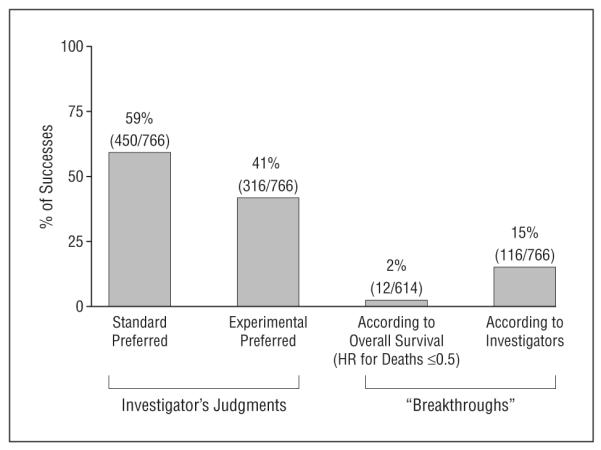
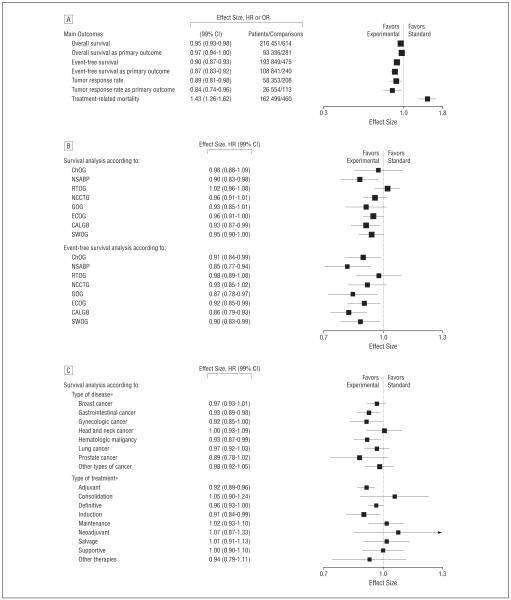
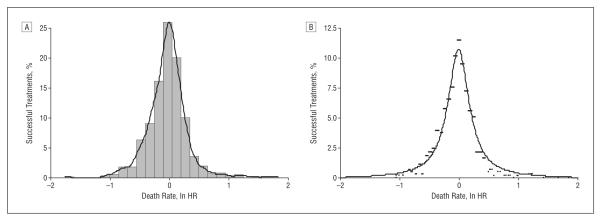
Results: Data from 624 trials (781 randomized comparisons) involving 216 451 patients were analyzed. In all, 30% of trials had statistically significant results, of which new interventions were superior to established treatments in 80% of trials. The original researchers judged that the risk-benefit profile favored new treatments in 41% of comparisons (316 of 766). Hazard ratios for overall and event-free survival, available for 614 comparisons, were 0.95 (99% confidence interval [CI], 0.93-0.98) and 0.90 (99% CI, 0.87- 0.93), respectively, slightly favoring new treatments. Breakthrough interventions were discovered in 15% of trials.
Conclusions: Approximately 25% to 50% of new cancer treatments that reach the stage of assessment in RCTs will prove successful. The pattern of successes has become more stable over time. The results are consistent with the hypothesis that the ethical principle of equipoise defines limits of discoverability in clinical research and ultimately drives therapeutic advances in clinical medicine.
Figures
Comment in
-
Cooperative groups are not..Arch Intern Med. 2008 Oct 27;168(19):2172-3; author reply 2173-4. doi: 10.1001/archinte.168.19.2172-b. Arch Intern Med. 2008. PMID: 18955657 No abstract available.
-
Treatment success in cancer.Arch Intern Med. 2008 Oct 27;168(19):2173; author reply 2173-4. doi: 10.1001/archinte.168.19.2173-a. Arch Intern Med. 2008. PMID: 18955658 No abstract available.
References
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007;57(1):43–66. - PubMed
-
- Wittes RE. Therapies for cancer in children: past successes, future challenges. N Engl J Med. 2003;348(8):747–749. - PubMed
-
- Collins R, McMahon S. Reliable assessment of the effects of treatment on mortality and major morbidity, I: clinical trials. Lancet. 2001;357(9253):373–380. - PubMed
-
- Grann A, Grann VR. The case for randomized trials in cancer treatment: new is not always better. JAMA. 2005;293(8):1001–1003. - PubMed
-
- National Cancer Institute 2005 Fact Book. [Accessed April 17, 2007]. http://fmb.cancer.gov/financial/attachments/FY-2005-FACT-BOOK-FINAL.pdf.
