

Upper airway surface tension but not upper airway collapsibility is elevated in primary Sjögren's syndrome
- PMID: 18363313
- PMCID: PMC2276736
- DOI: 10.1093/sleep/31.3.367
Upper airway surface tension but not upper airway collapsibility is elevated in primary Sjögren's syndrome
Abstract
Study objectives: Primary Sjögren's syndrome is an autoimmune disease typified by xerostomia (dry mouth) that, in turn, could lead to increased saliva surface tension (gamma) and increased upper airway collapsibility. Fatigue, of unknown etiology, is also frequently reported by patients with primary Sjögren's syndrome. Recent preliminary data indicate a high prevalence of obstructive sleep apnea in healthy-weight women with primary Sjögren's syndrome. Concurrent research highlights a significant role of gamma in the maintenance of upper airway patency. The aim of this study was to compare oral mucosal wetness, saliva gamma, and upper airway collapsibility during wake and sleep between women with primary Sjögren's syndrome and matched control subjects.
Setting: Participants slept in a sound-insulated room with physiologic measurements controlled from an adjacent room.
Participants: Eleven women with primary Sjögren's syndrome and 8 age- and body mass index-matched control women.
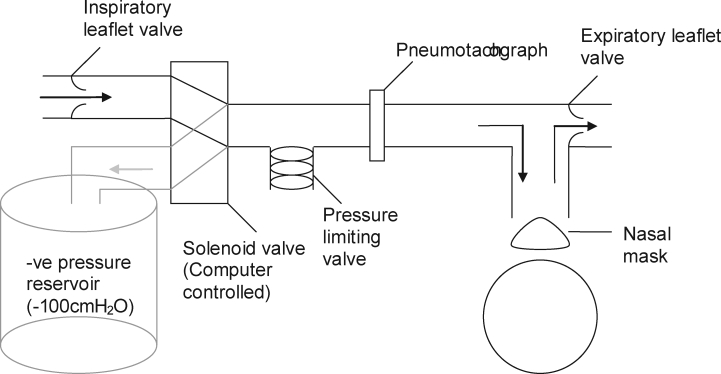
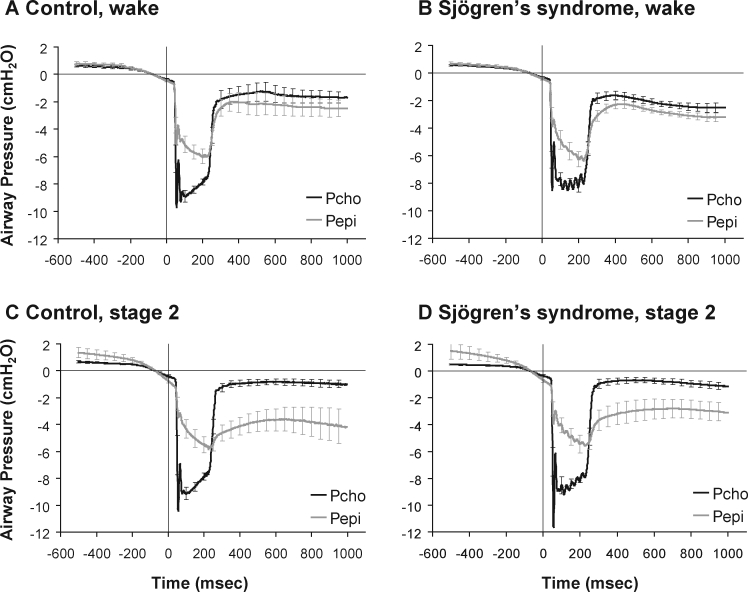
Interventions: Upper airway collapsibility index (minimum choanal-epiglottic pressure expressed as a percentage of delivered choanal pressure) was determined from brief negative-pressure pulses delivered to the upper airway during early inspiration in wakefulness and sleep.
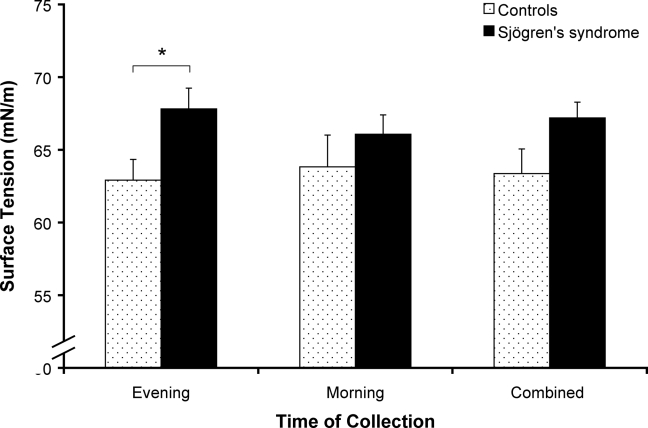
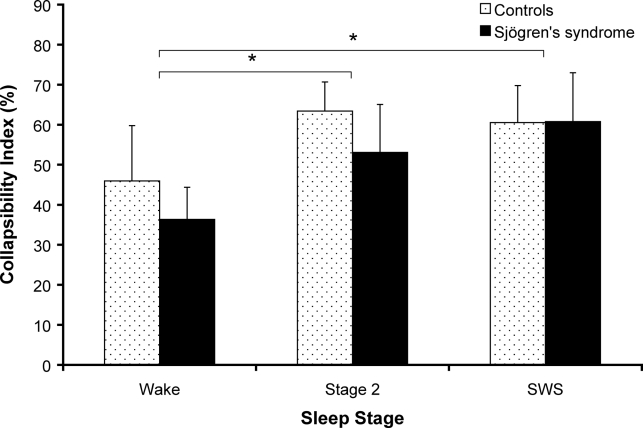
Measurements and results: Patients with primary Sjögren's syndrome had significantly higher saliva gamma ("pull-off" force method) compared with control subjects (67.2 +/- 1.1 mN/m versus 63.2 +/- 1.7 mN/m, P < 0.05). Upper airway collapsibility index significantly increased from wake to sleep (Stage 2 and slow wave sleep) but was not different between groups during wake (primary Sjögren's syndrome versus controls; 36.3% +/- 8.0% vs 46.0 +/- 13.8%), stage 2 sleep (53.1% +/- 11.9% vs 63.4% +/- 7.2%), or slow-wave sleep (60.8% +/- 12.2% vs 60.5% +/- 9.3%).
Conclusions: Despite having a significantly "stickier" upper airway, patients with primary Sjögren's syndrome do not appear to have abnormal upper airway collapsibility, at least as determined from upper airway collapsibility index.
Figures
References
-
- Kassan SS, Moutsopoulos HM. Clinical manifestations and early diagnosis of Sjogren syndrome. Arch Intern Med. 2004 Jun 28;164:1275–1284. - PubMed
-
- Venables PJ. Sjogren's syndrome. Best Pract Res Clin Rheumatol. 2004;18:313–329. - PubMed
-
- Thomas E, Hay EM, Hajeer A, Silman AJ. Sjogren's syndrome: a community-based study of prevalence and impact. Br J Rheumatol. 1998;37:1069–1076. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
