

Reproducibility and validity of a handheld spirometer
- PMID: 18364054
- PMCID: PMC3595551
Reproducibility and validity of a handheld spirometer
Abstract
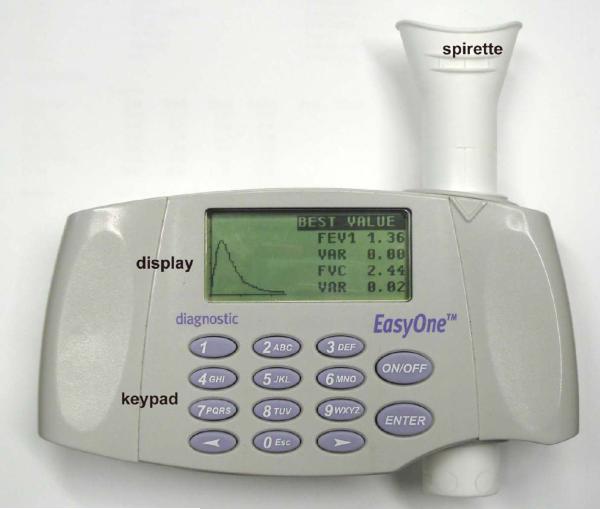
Background: Handheld spirometers have several advantages over desktop spirometers, but worries persist regarding reproducibility and validity of data from handheld spirometers. We undertook an independent examination of the EasyOne handheld spirometer.
Methods: The laboratory testing included reproducibility and validity testing with a waveform generator. We used standard American Thoracic Society waveforms for in-line testing, calibration adaptor testing, and testing during compression of the mouthpiece. The clinical testing involved repeated tests with 24 spirometry-naïve volunteers and comparison to spirometry results from laboratory (volume-sensing dry rolling seal) spirometer.
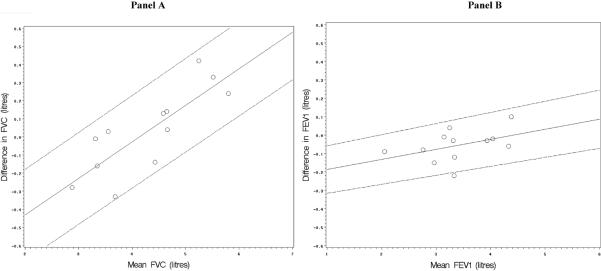
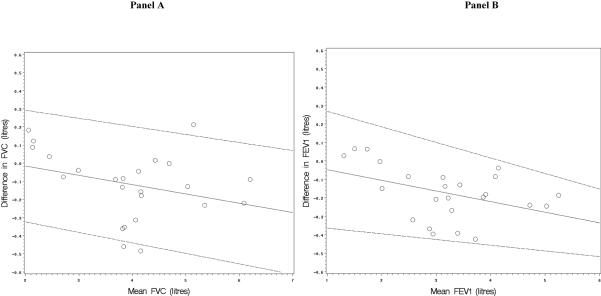
Results: The EasyOne exceeded standard thresholds for acceptability with the American Thoracic Society waveforms. In-line testing yielded valid results from the EasyOne. Between the EasyOne and the reference spirometer readings the mean +/- SD difference was 0.03 +/- 0.23 L for forced vital capacity (FVC) and -0.06 +/- 0.09 L for forced expiratory volume in the first second (FEV(1)). The calibration adaptor showed no appreciable problems. Extreme compression of the mouthpiece reduced the measured values. In clinical testing the coefficients of variation and limits of agreement were, respectively, 3.3% and 0.24 L for FVC, 2.6% and 0.18 L for FEV(1), and 1.9% and 0.05 for the FEV(1)/FVC ratio. The EasyOne readings were lower than those from the reference spirometer; the differences were: -0.12 L for FVC, -0.17 L for FEV(1), and -0.02 for FEV(1)/FVC. The limits of agreement were within criteria for FVC but not for the FEV(1), possibly due to a training effect.
Conclusion: The EasyOne spirometer yielded generally reproducible results that were generally valid, compared to the values from the laboratory spirometer. The use of the EasyOne in clinical, occupational, and research settings seems justified.
Figures

Comment in
-
Documentation of airflow obstruction is essential to confirm the diagnosis of COPD: are handheld spirometers in an office setting valid?Respir Care. 2008 Apr;53(4):429-30. Respir Care. 2008. PMID: 18364052 No abstract available.
Similar articles
-
Performance of a new screening spirometer at a community health fair.Respir Care. 2002 Oct;47(10):1150-7. Respir Care. 2002. PMID: 12354333
-
Agreement between spirometers: a challenge in the follow-up of patients and populations?Respiration. 2013;85(6):505-14. doi: 10.1159/000346649. Epub 2013 Mar 8. Respiration. 2013. PMID: 23485575 Clinical Trial.
-
Clinical Validation of the Spirohome Clinic Ultrasonic Spirometer in Child and Adolescent Patients.J Asthma Allergy. 2022 Feb 15;15:219-229. doi: 10.2147/JAA.S345189. eCollection 2022. J Asthma Allergy. 2022. PMID: 35210788 Free PMC article.
-
Comparison of a new desktop spirometer (Spirospec) with a laboratory spirometer in a respiratory out-patient clinic.Respir Care. 2003 Jun;48(6):591-5. Respir Care. 2003. PMID: 12780945 Clinical Trial.
-
Stability of the EasyOne ultrasonic spirometer for use in general practice.Respirology. 2006 May;11(3):306-10. doi: 10.1111/j.1440-1843.2006.00842.x. Respirology. 2006. PMID: 16635089
Cited by
-
Lung Function Testing and Prediction Equations in Adult Population from Maputo, Mozambique.Int J Environ Res Public Health. 2020 Jun 24;17(12):4535. doi: 10.3390/ijerph17124535. Int J Environ Res Public Health. 2020. PMID: 32599726 Free PMC article.
-
Asthma management in the digital age.Front Allergy. 2024 Sep 3;5:1451768. doi: 10.3389/falgy.2024.1451768. eCollection 2024. Front Allergy. 2024. PMID: 39291253 Free PMC article. Review.
-
Randomised controlled trial with parallel process evaluation and health economic analysis to evaluate a nutritional management intervention, OptiCALS, for patients with amyotrophic lateral sclerosis: study protocol.BMJ Open. 2025 May 27;15(5):e096098. doi: 10.1136/bmjopen-2024-096098. BMJ Open. 2025. PMID: 40436457 Free PMC article.
-
Validation of the portable Bluetooth® Air Next spirometer in patients with different respiratory diseases.Respir Res. 2020 Apr 6;21(1):79. doi: 10.1186/s12931-020-01341-z. Respir Res. 2020. PMID: 32252783 Free PMC article.
-
Health inequity: Possibilities of initiating pulmonary telerehabilitation programs for adults with chronic obstructive pulmonary disorders in conflict and low-resourced areas; A mixed-method phenomenological study.PLoS One. 2025 May 29;20(5):e0324624. doi: 10.1371/journal.pone.0324624. eCollection 2025. PLoS One. 2025. PMID: 40440329 Free PMC article.
References
-
- Mannino DM, et al. Chronic obstructive pulmonary disease surveillance -- United States, 1971–2000. Surveillance Summaries, August 2, 2002. MMWR. 2002;51(SS-6):1–8. - PubMed
-
- Ferguson GT, et al. Office spirometry for lung health assessment in adults: A consensus statement from the National Lung Health Education Program. Chest. 2000;117:1146–61. - PubMed
-
- Enright PL, Kaminsky DA. Strategies for screening for chronic obstructive pulmonary disease. Respir Care. 2003;48:1194–1201. - PubMed
-
- Hankinson JL. Beyond the peak flow meter: newer technologies for determining and documenting changes in lung function in the workplace. Occupational Medicine. 2000;15(2):411–20. - PubMed
-
- Enright P. Spirometers' technological evolution spurs increased confidence in results. Four generations of advances enable more useful diagnoses for asthma, emphysema or tuberculosis. Occup Health Saf. 1994;63:81–84. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical