

The efficacy of pharmacotherapy for decreasing the expansion rate of abdominal aortic aneurysms: a systematic review and meta-analysis
- PMID: 18365027
- PMCID: PMC2267254
- DOI: 10.1371/journal.pone.0001895
The efficacy of pharmacotherapy for decreasing the expansion rate of abdominal aortic aneurysms: a systematic review and meta-analysis
Abstract
Background: Pharmacotherapy may represent a potential means to limit the expansion rate of abdominal aortic aneurysms (AAAs). Studies evaluating the efficacy of different pharmacological agents to slow down human AAA-expansion rates have been performed, but they have never been systematically reviewed or summarized.
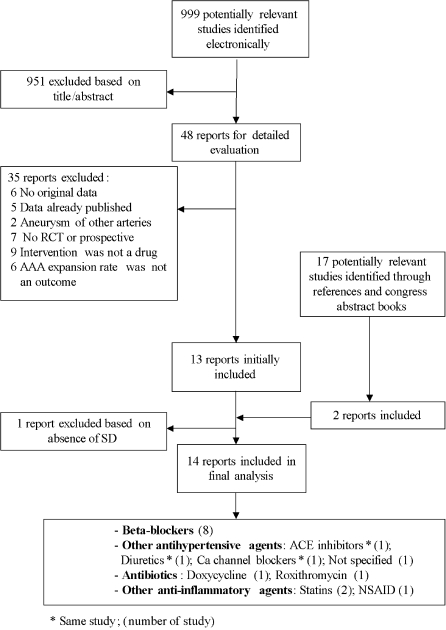
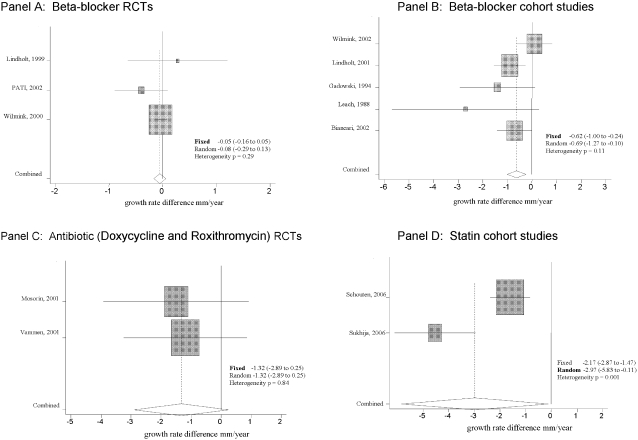
Methods and findings: Two independent reviewers identified studies and selected randomized trials and prospective cohort studies comparing the growth rate of AAA in patients with pharmacotherapy vs. no pharmacotherapy. We extracted information on study interventions, baseline characteristics, methodological quality, and AAA growth rate differences (in mm/year). Fourteen prospective studies met eligibility criteria. Five cohort studies raised the possibility of benefit of beta-blockers [pooled growth rate difference: -0.62 mm/year, (95%CI, -1.00 to -0.24)], but this was not confirmed in three beta-blocker RCTs [pooled RCT growth rate difference: -0.05 mm/year (-0.16 to 0.05)]. Statins have been evaluated in two cohort studies that yield a pooled growth rate difference of -2.97 (-5.83 to -0.11). Doxycycline and roxithromycin have been evaluated in two RCTs that suggest possible benefit [pooled RCT growth rate difference: -1.32 mm/year (-2.89 to 0.25)]. Studies assessing NSAIDs, diuretics, calcium channel blockers and ACE inhibitors, meanwhile, did not find statistically significant differences.
Conclusions: Beta-blockers do not appear to significantly reduce the growth rate of AAAs. Statins and other anti-inflammatory agents appear to hold promise for decreasing the expansion rate of AAA, but need further evaluation before definitive recommendations can be made.
Conflict of interest statement
Figures
References
-
- Fleming C, Whitelock EP, Beil TL, Lederle FA. Screenning for abdominal aortic aneurysm: a best-evidence systematic review for the U.S Preventive Sevices task Force. Ann Intern Med. 2005;142:203–11. - PubMed
-
- Lederle FA, Wilson SE, Johnson GR, Reinke DB, Littooy FN, et al. Aneurysm Detection and Management Veterans Affairs Cooperative Study Group. Immediate repair compared with surveillance of small abdominal aortic aneurysms. N Engl J Med. 2002;346:1437–44. - PubMed
-
- The UK Small Aneurysm trial Participants. Mortality results for randomised controlled trial of early elective surgery or ultrasonographic surveillance for small abdominal aortic aneurysm. Lancet. 1998;352:1649–1655. - PubMed
-
- Guessous I, Cornuz J. Abdominal aortic aneurysm screening: 2006 recommendations. Expert Rev Pharmacoeconomics Outcomes Res. 2006;6:555–561. - PubMed
-
- Scott RA, Thompson SG. Screening, surgical repair, and the management of abdominal aortic aneurisms. J Med Screen. 2005;12:57–58. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
