

Chronic administration of nevirapine during pregnancy: impact of pregnancy on pharmacokinetics
- PMID: 18366444
- PMCID: PMC2755564
- DOI: 10.1111/j.1468-1293.2008.00553.x
Chronic administration of nevirapine during pregnancy: impact of pregnancy on pharmacokinetics
Abstract
Objectives: To determine the impact of pregnancy on the pharmacokinetics (PK) of nevirapine (NVP) during chronic dosing in HIV-infected women and appropriate NVP dosing in this population.
Methods: Twenty-six pregnant women participating in two open-label Pediatric AIDS Clinical Trials Group studies (P1022 and P1026S) were evaluated. Each patient received 200 mg NVP every 12 h and had PK evaluations during the second or third trimester; these evaluations were repeated postpartum. Paired maternal and cord blood NVP concentrations were collected at delivery in nine patients. Ante- and postpartum comparisons were made using paired t-tests and using a 'bioequivalence' approach to determine confidence interval (CI).
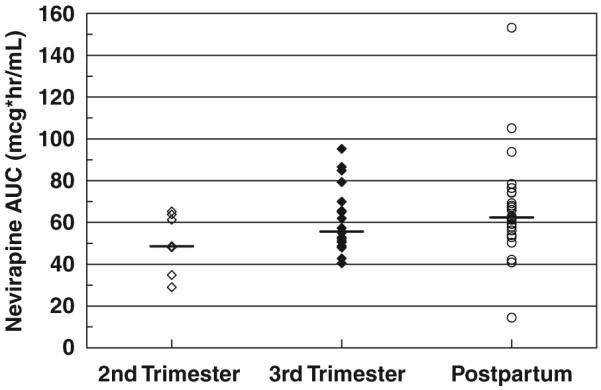
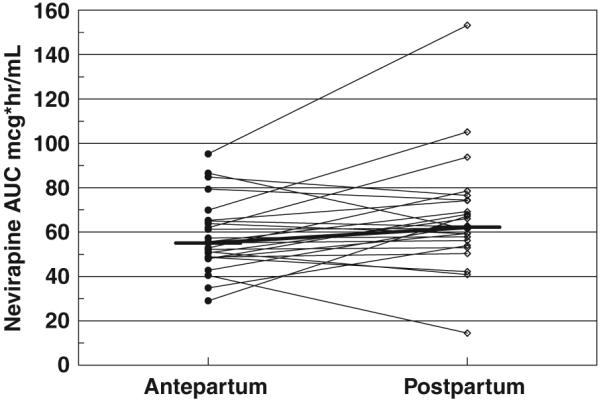
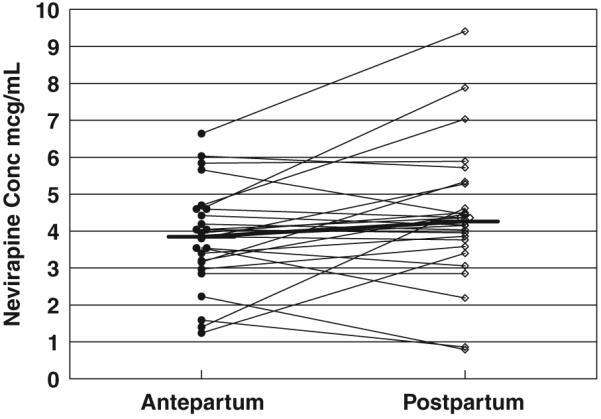
Results: The average NVP Area Under the Curve (AUC) was 56 +/- 13 mcg(*)h/mL antepartum and 61 +/- 15 mcg(*)h/mL postpartum. The typical parameters +/- standard error were apparent clearance (CL/F)=3.51 +/- 0.18 L/h and apparent volume of distribution (Vd/F)=121 +/- 19.8 L. There were no significant differences between antepartum and postpartum AUC or pre-dose concentrations. The AUC ratio was 0.90 with a 90% CI of the mean equal to 0.80-1.02. The median (+/- standard deviation) cord blood to maternal NVP concentration ratio was 0.91 +/- 0.90.
Conclusions: Pregnancy does not alter NVP PK and the standard dose (200 mg every 12 h) is appropriate during pregnancy.
Figures
References
-
- Mofenson LM, Lambert JS, Stiehm ER, et al. Pediatric AIDS Clinical Trials Group Study 185 Team Risk factors for perinatal transmission of human immunodeficiency virus type 1 in women treated with zidovudine. N Engl J Med. 1999;341:385–393. - PubMed
-
- Saitoh A, Hull AD, Franklin P, Spector SA. Myelomeningocele in an infant with intrauterine exposure to efavirenz. J Perinatol. 2005;25:555–556. - PubMed
-
- Lyons F, Hopkins S, Kelleher B, et al. Maternal hepatotoxicity with nevirapine as part of combination antiretroviral therapy in pregnancy. HIV Med. 2006;7:255–260. - PubMed
-
- Hitti J, Frenkel LM, Stek AM, et al. Maternal toxicity with continuous nevirapine in pregnancy: results from PACTG 1022. J Acquir Immune Defic Syndr. 2004;36:772–776. - PubMed
-
- Acosta EP, Zorrilla C, Van Dyke R, et al. Pharmacokinetics of saquinavir - SGC in HIV-infected pregnant women. HIV Clin Trials. 2001;2:460–465. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
