

Failure to achieve a complete response to induction BCG therapy is associated with increased risk of disease worsening and death in patients with high risk non-muscle invasive bladder cancer
- PMID: 18367117
- PMCID: PMC2695968
- DOI: 10.1016/j.urolonc.2007.11.033
Failure to achieve a complete response to induction BCG therapy is associated with increased risk of disease worsening and death in patients with high risk non-muscle invasive bladder cancer
Abstract
Purpose: The Southwest Oncology Group conducted a randomized trial of induction bacillus Calmette-Guérin (BCG) with or without maintenance BCG. In these additional retrospective analyses, our goal was to evaluate the association of a complete response (CR) or remaining with no evidence of disease (NED) vs. no CR during induction therapy with subsequent survival after adjusting for other potential confounders. Among all patients randomized to maintenance treatment, we also wanted to identify combinations of baseline covariates in order to define prognostic groups for subsequent worsening-free survival.
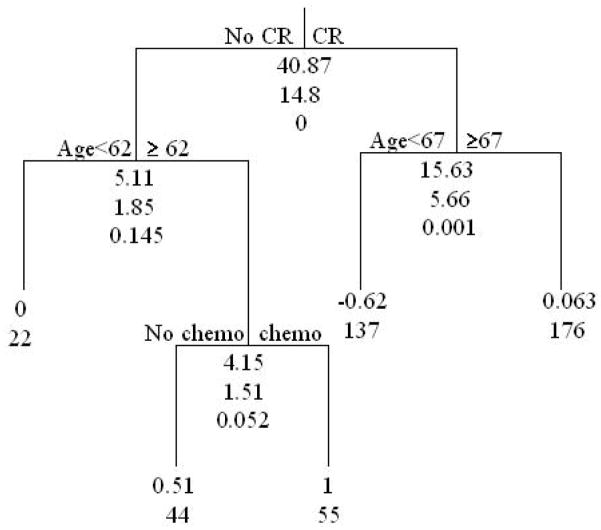
Methods: Outcome measures of worsening-free and overall survival were assessed using Kaplan Meier estimates and proportional hazards regression models. For the classification and regression tree (CART) analysis, 434 patients randomized to maintenance vs. no therapy with complete covariate information were included.
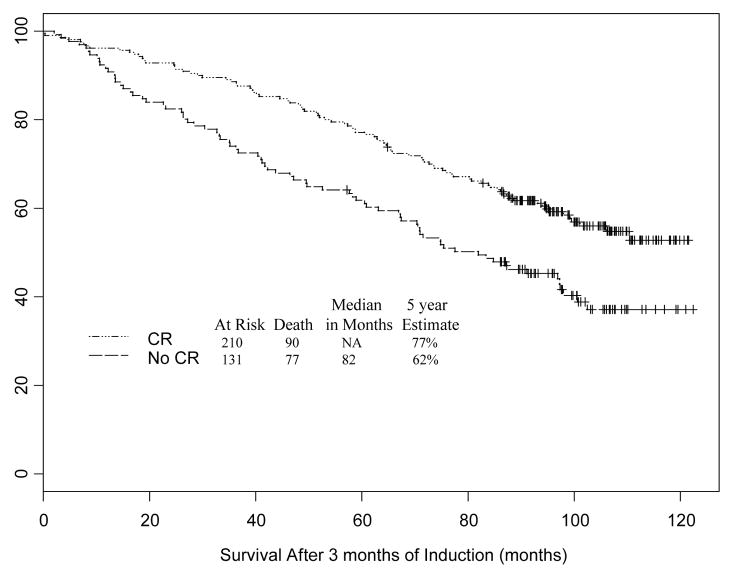
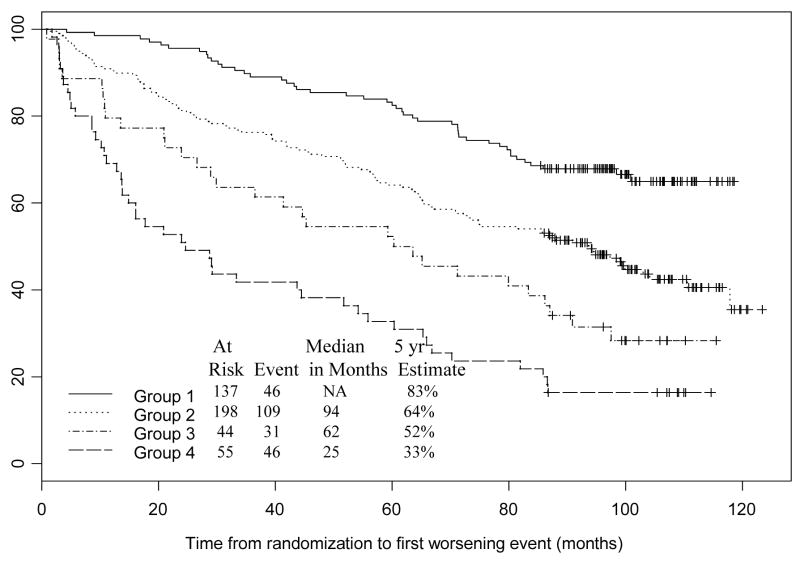
Results: Of the 593 evaluable patients, 341 were not randomized to maintenance BCG. Patients who achieved a prior complete response during induction BCG had a 5-year survival probability of 77% compared with 62% for patients who did not [hazard ratio (HR) 0.60; 95% confidence interval (CI) 0.44, 0.81; P = 0.0008]. Prior CR retained significance when adjusted for age, gender, prior intravesical chemotherapy, and papillary disease versus CIS (HR = 0.63; 95% CI: 0.46, 0.86; P = 0.003). CART analysis identified 4 prognostic groups. Older patients (> or =62 years old) previously treated with intravesical chemotherapy who failed to achieve a CR had a 5-fold higher risk of a worsening event relative to those who are younger (<67 years old) and achieve a CR (HR = 5.09; 95% CI: 3.37, 7.68; P < 0.0001).
Conclusion: Failure to achieve a complete response after induction BCG is associated with a significant risk of a worsening event and death for patients with CIS or Ta or T1 bladder cancer at increased risk of recurrence.
Figures
References
-
- Kelley DR, Ratliff TL, Catalona WJ, Shapiro A, Lage JM, Bauer WC, et al. Intravesical bacillus Calmette-Guerin therapy for superficial bladder cancer: effect of bacillus Calmette-Guerin viability on treatment results. J Urol. 1985;134(1):48–53. - PubMed
-
- Herr HW, Schwalb DM, Zhang ZF, Sogani PC, Fair WR, Whitmore WF, Jr, et al. Intravesical bacillus Calmette-Guerin therapy prevents tumor progression and death from superficial bladder cancer: ten-year follow-up of a prospective randomized trial. J Clin Oncol. 1995;13(6):1404–8. - PubMed
-
- Cookson MS, Sarosdy MF. Management of stage T1 superficial bladder cancer with intravesical bacillus Calmette-Guerin therapy. J Urol. 1992;148(3):797–801. - PubMed
-
- Lamm DL, Blumenstein BA, Crissman JD, Montie JE, Gottesman JE, Lowe BA, et al. Maintenance bacillus Calmette-Guerin immunotherapy for recurrent TA, T1 and carcinoma in situ transitional cell carcinoma of the bladder: a randomized Southwest Oncology Group Study. J Urol. 2000;163(4):1124–9. - PubMed
-
- Esuvaranathan K, Kamaraj R, Mohan RS, Cheng C, Tan PK, Tay KP, et al. A phase IIB trial of BCG combined with interferon alpha for bladder cancer. J Urol. 2000;163(4 Supplement) Abstract # 675.
Publication types
MeSH terms
Substances
Grants and funding
- N01 CA032102/CA/NCI NIH HHS/United States
- 1UO1CA77150-01/CA/NCI NIH HHS/United States
- M01 RR000188/RR/NCRR NIH HHS/United States
- R01 CA071921/CA/NCI NIH HHS/United States
- 5 R01 CA098897 04/CA/NCI NIH HHS/United States
- 1R01CA71921-01/CA/NCI NIH HHS/United States
- U10 CA032102/CA/NCI NIH HHS/United States
- 2PC50CA091846-06S2/CA/NCI NIH HHS/United States
- N01 CA038926/CA/NCI NIH HHS/United States
- U10 CA038926/CA/NCI NIH HHS/United States
- 5 R01 CA074880 08/CA/NCI NIH HHS/United States
- N01 CN085186/CA/NCI NIH HHS/United States
- P50 CA091846/CA/NCI NIH HHS/United States
- R01 CA074880/CA/NCI NIH HHS/United States
- N01-CN-85186/CN/NCI NIH HHS/United States
- R01 CA098897/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
