

Endoscopic tri-modal imaging for surveillance in ulcerative colitis: randomised comparison of high-resolution endoscopy and autofluorescence imaging for neoplasia detection; and evaluation of narrow-band imaging for classification of lesions
- PMID: 18367559
- PMCID: PMC2564833
- DOI: 10.1136/gut.2007.144097
Endoscopic tri-modal imaging for surveillance in ulcerative colitis: randomised comparison of high-resolution endoscopy and autofluorescence imaging for neoplasia detection; and evaluation of narrow-band imaging for classification of lesions
Abstract
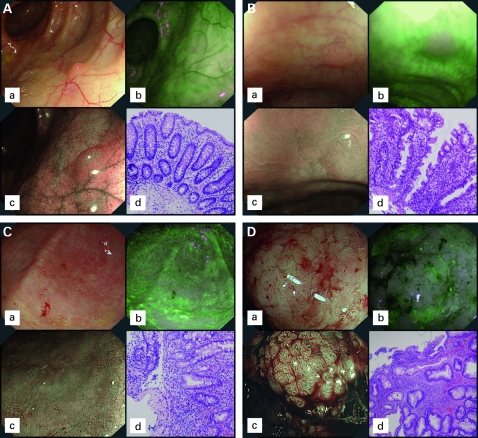
Background: Endoscopic tri-modal imaging (ETMI) incorporates white light endoscopy (WLE), autofluorescence imaging (AFI) and narrow-band imaging (NBI).
Aims: To assess the value of ETMI for the detection and classification of neoplasia in patients with longstanding ulcerative colitis.
Design: Randomised comparative trial of tandem colonoscopies.
Setting: Academic Medical Centre Amsterdam, Netherlands.
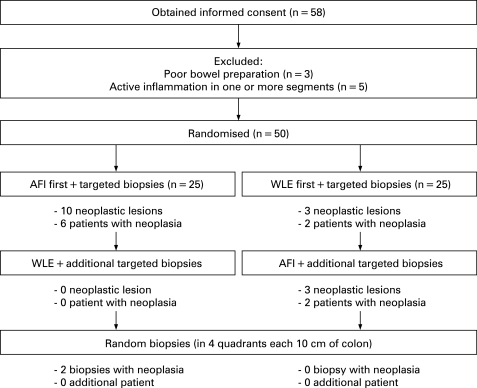
Patients and methods: Fifty patients with ulcerative colitis underwent surveillance colonoscopy with ETMI. Each colonic segment was inspected twice, once with AFI and once with WLE, in random order. All detected lesions were inspected by NBI for Kudo pit pattern analysis and additional random biopsies were taken.
Main outcome measures: Neoplasia miss-rates of AFI and WLE, and accuracy of the Kudo classification by NBI.
Results: Among patients assigned to inspection with AFI first (n = 25), 10 neoplastic lesions were primarily detected. Subsequent WLE detected no additional neoplasia. Among patients examined with WLE first (n = 25), three neoplastic lesions were detected; subsequent inspection with AFI added three neoplastic lesions. Neoplasia miss-rates for AFI and WLE were 0% and 50% (p = 0.036). The Kudo classification by NBI had a sensitivity and specificity of 75% and 81%; however, all neoplasia was coloured purple on AFI (sensitivity 100%). No additional patients with neoplasia were detected by random biopsies.
Conclusion: Autofluorescence imaging improves the detection of neoplasia in patients with ulcerative colitis and decreases the yield of random biopsies. Pit pattern analysis by NBI has a moderate accuracy for the prediction of histology, whereas AFI colour appears valuable in excluding the presence of neoplasia.
Trial registration number: ISRCTN05272746.
Conflict of interest statement
Figures
References
-
- Itzkowitz SH, Harpaz N. Diagnosis and management of dysplasia in patients with inflammatory bowel diseases. Gastroenterology 2004;126:1634–48 - PubMed
-
- Collins P, Mpofu C, Watson A, et al. Strategies for detecting colon cancer and/or dysplasia in patients with inflammatory bowel disease. Cochrane Database Syst Rev 2006;(2):CD000279. - PubMed
-
- Itzkowitz SH, Present DH. Consensus conference: Colorectal cancer screening and surveillance in inflammatory bowel disease. Inflamm Bowel Dis 2005;11:314–21 - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical