

The affective dimension of laboratory dyspnea: air hunger is more unpleasant than work/effort
- PMID: 18369200
- PMCID: PMC2427058
- DOI: 10.1164/rccm.200711-1675OC
The affective dimension of laboratory dyspnea: air hunger is more unpleasant than work/effort
Abstract
Rationale: It is hypothesized that the affective dimension of dyspnea (unpleasantness, emotional response) is not strictly dependent on the intensity of dyspnea.
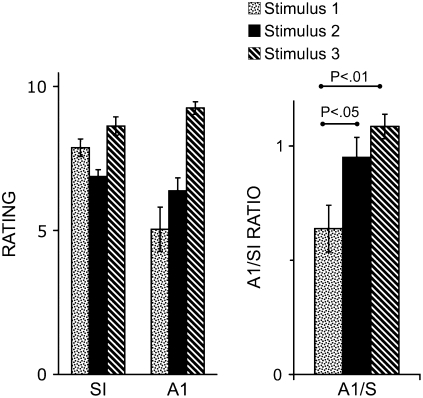
Objectives: We tested the hypothesis that the ratio of immediate unpleasantness (A(1)) to sensory intensity (SI) varies depending on the type of dyspnea.
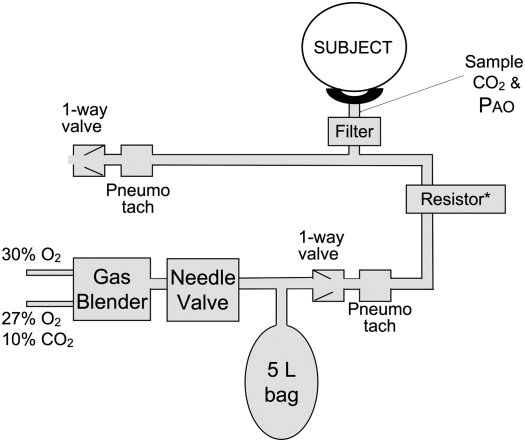
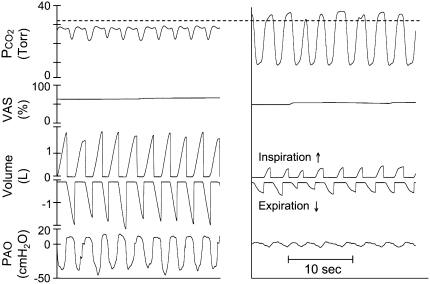
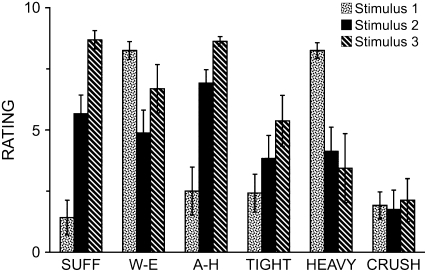
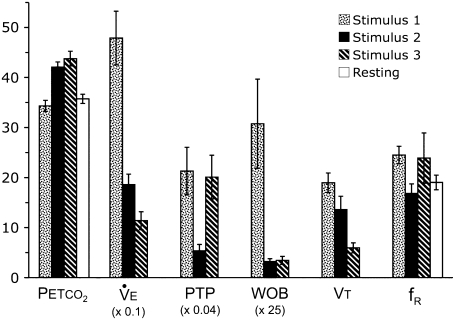
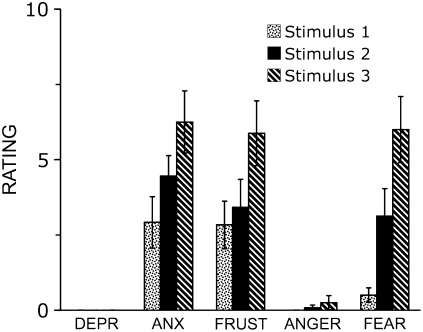
Methods: Twelve healthy subjects experienced three stimuli: stimulus 1: maximal eucapnic voluntary hyperpnea against inspiratory resistance, requiring 15 times the work of resting breathing; stimulus 2: Pet(CO(2)) 6.1 mm Hg above resting with ventilation restricted to less than spontaneous breathing; stimulus 3: Pet(CO(2)) 7.7 mm Hg above resting with ventilation further restricted. After each trial, subjects rated SI, A(1), and qualities of dyspnea on the Multidimensional Dyspnea Profile (MDP), a comprehensive instrument tested here for the first time.
Measurements and main results: Stimulus 1 was always limited by subjects failing to meet a higher ventilation target; none signaled severe discomfort. This evoked work and effort sensations, with relatively low unpleasantness (mean A(1)/SI = 0.64). Stimulus 2, titrated to produce dyspnea ratings similar to those subjects gave during stimulus 1, evoked air hunger and produced significantly greater unpleasantness (mean A(1)/SI = 0.95). Stimulus 3, increased until air hunger was intolerable, evoked the highest intensity and unpleasantness ratings and high unpleasantness ratio (mean A(1)/SI = 1.09). When asked which they would prefer to repeat, all subjects chose stimulus 1.
Conclusions: (1) Maximal respiratory work is less unpleasant than moderately intense air hunger in this brief test; (2) unpleasantness of dyspnea can vary independently from perceived intensity, consistent with the prevailing model of pain; (3) separate dimensions of dyspnea can be measured with the MDP.
Figures
References
-
- American Thoracic Society. Dyspnea: mechanisms, assessment, and management: a consensus statement. Am J Respir Crit Care Med 1999;159:321–340. - PubMed
-
- International Association for the Study of Pain Task Force on Taxonomy. Classification of chronic pain. In: Merskey H, Bogduk N, editors. Classification of chronic pain, 2nd ed. Seattle, WA: IASP Press; 1994. p. 210.
-
- Dudgeon DJ. Managing dyspnea and cough. Hematol Oncol Clin North Am 2002;16:557–577. - PubMed
-
- Price DD. Psychological and neural mechanisms of the affective dimension of pain. Science 2000;288:1769–1772. - PubMed
-
- Price DD, Harkins SW. The affective-motivational dimension of pain: a two-stage model. APS Journal 1992;1:229–239.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
