

High-risk prostate cancer in the United States, 1990-2007
- PMID: 18369637
- PMCID: PMC2948572
- DOI: 10.1007/s00345-008-0250-7
High-risk prostate cancer in the United States, 1990-2007
Abstract
Objectives: This study aimed to describe national trends in presentation, management, and outcomes for men with high risk prostate cancer.
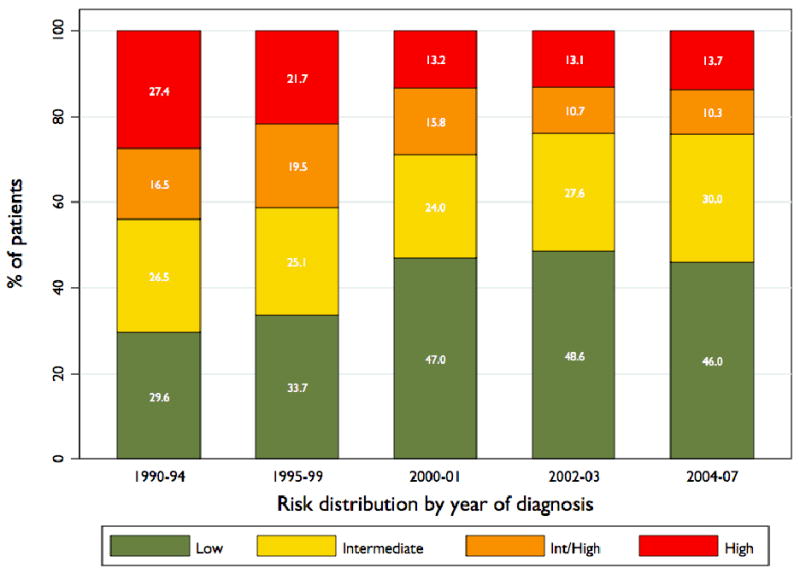
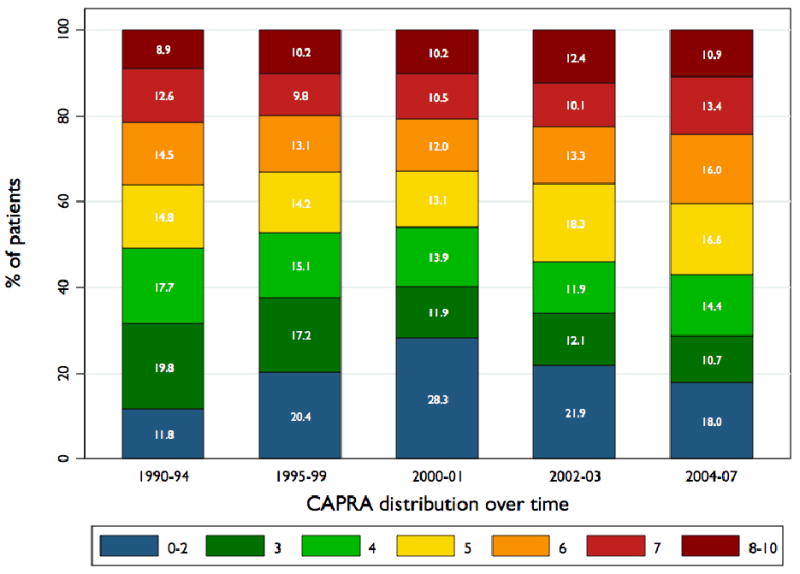
Methods: Data were abstracted from CaPSURE; 10,808 men were diagnosed between 1990 and 2007 and had complete clinical data. High-risk was defined according to the D'Amico criteria; a more restrictive definition assigned clinical stage T2c to intermediate rather than high risk. Temporal trends were assessed for patient distribution among risk groups, and within the high-risk group for individual risk factors, Kattan nomogram score, Cancer of the Prostate Risk Assessment (CAPRA) score, and primary treatment. Survival analysis stratified by CAPRA score was performed.
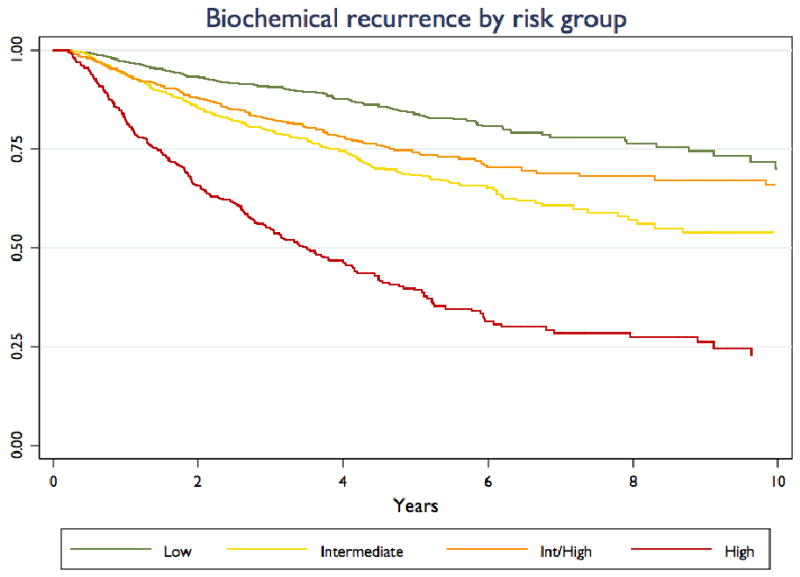
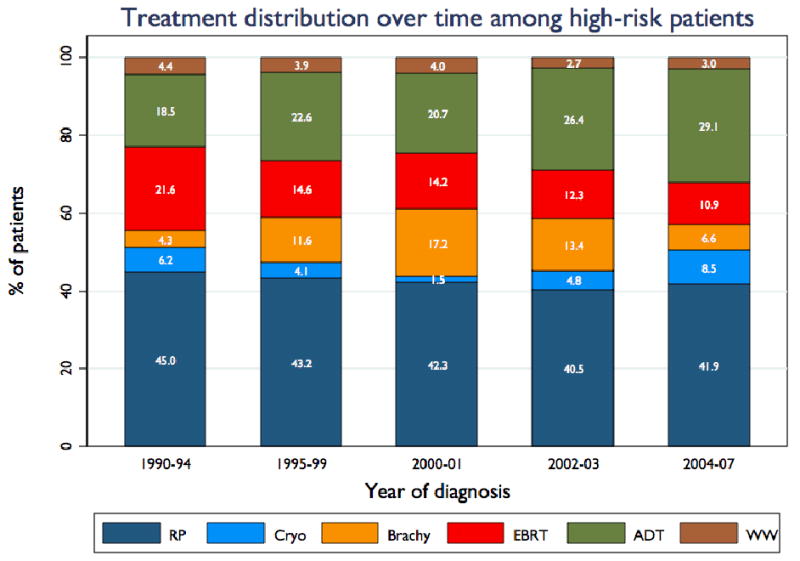
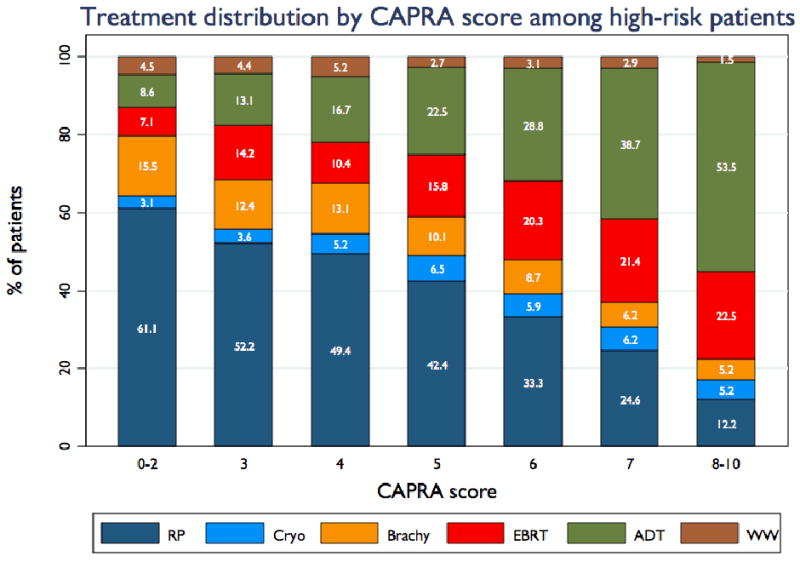
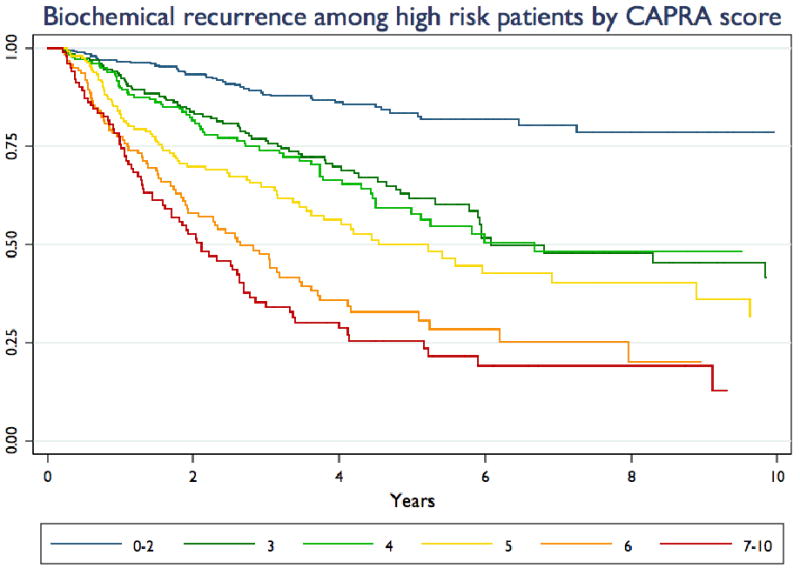
Results: Under the standard definition, 31.2% of the men were diagnosed with high-risk disease, and 16.9% were high-risk under the restrictive definition. This proportion has fallen over time but has been stable since 2000. Patients who would be stratified to high risk under the standard definition and to intermediate risk under the restrictive definition have better outcomes than those stratified to either intermediate or high risk under both definitions. There has been no consistent risk migration within the high-risk group over time. Treatment varies substantially with CAPRA score within the high-risk group, with higher risk men less likely to receive local therapy. Use of androgen deprivation therapy has increased over time, both as primary therapy and in conjunction with both external beam radiation and brachytherapy. Biochemical outcomes vary according to CAPRA score within the high-risk group.
Conclusions: Clinical stage T2c should not define high risk, and the high-risk group should be substratified using a multivariable instrument. There is no evidence for meaningful downward risk migration among high-risk patients over the past 15 years. At least some men in the high-risk group may be undertreated.
Figures
References
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007;57:43–66. - PubMed
-
- Thompson IM. Defining high risk prostate cancer--where do we set the bar? A translational science approach to risk stratification. J Urol. 2006;176:S21–4. discussion S5-6. - PubMed
-
- Cooperberg MR, Freedland SJ, Pasta DJ, et al. Multiinstitutional validation of the UCSF cancer of the prostate risk assessment for prediction of recurrence after radical prostatectomy. Cancer. 2006;107:2384–91. - PubMed
-
- D'Amico AV, Whittington R, Malkowicz SB, et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA. 1998;280:969–74. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
