

WT1 expression distinguishes astrocytic tumor cells from normal and reactive astrocytes
- PMID: 18371184
- PMCID: PMC8095516
- DOI: 10.1111/j.1750-3639.2008.00127.x
WT1 expression distinguishes astrocytic tumor cells from normal and reactive astrocytes
Abstract
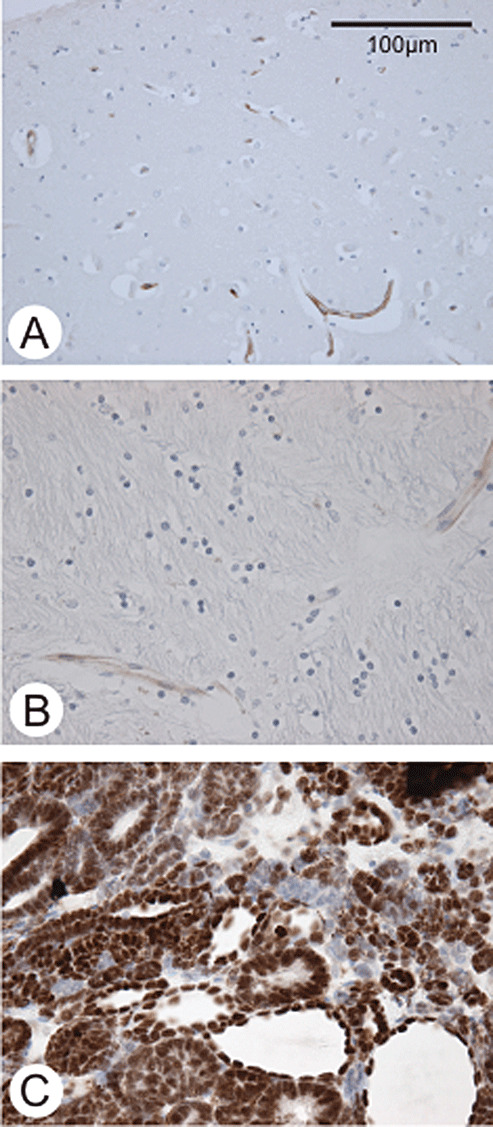
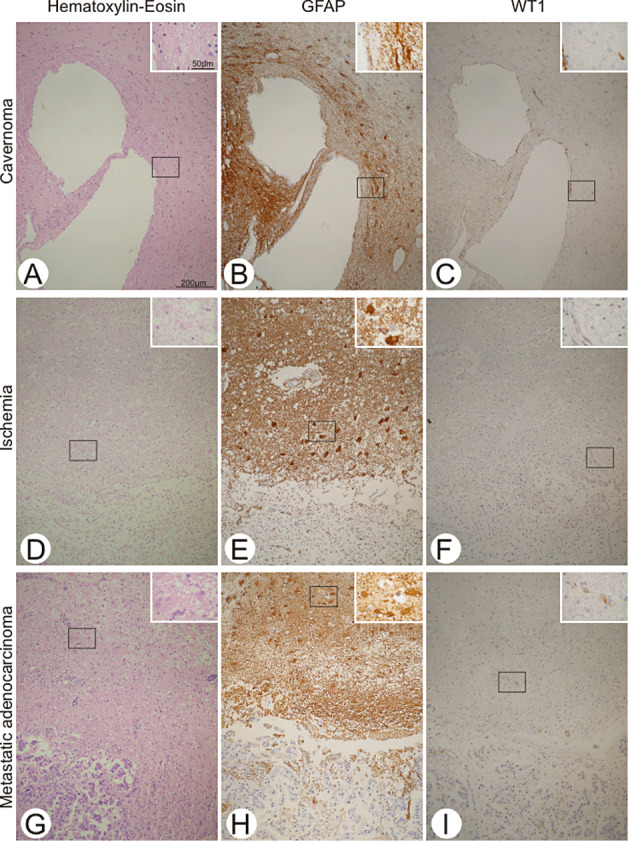
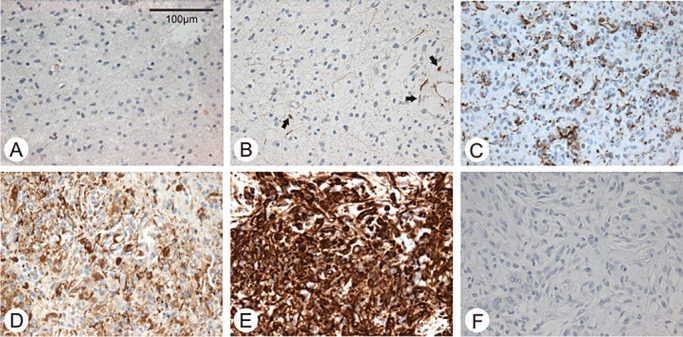
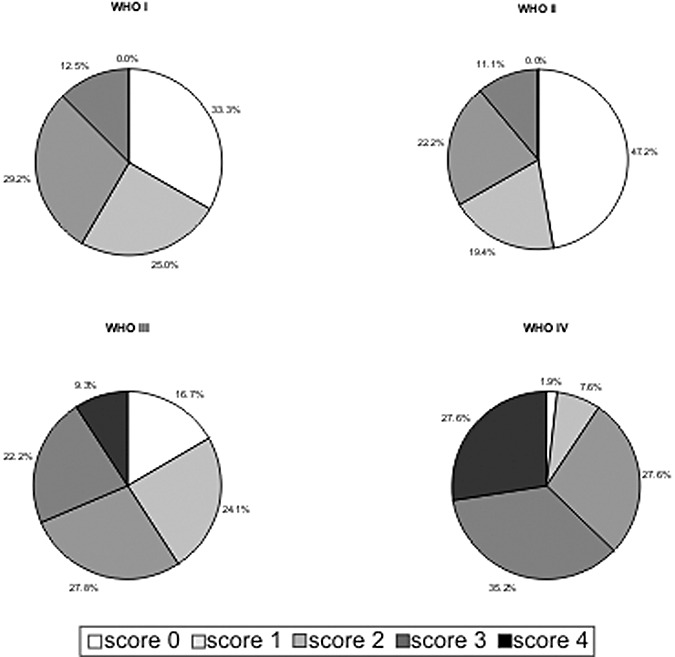
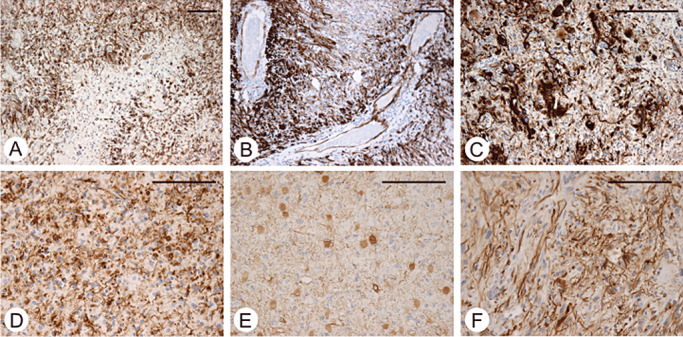
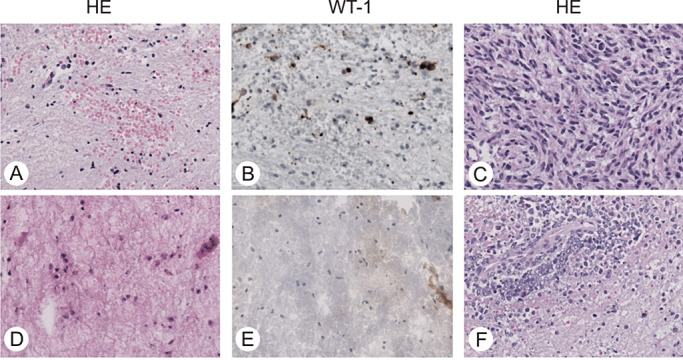
Particularly in small brain biopsies, it might be difficult to distinguish reactive astrogliosis from low-grade or infiltration zones of high-grade astrocytomas. So far no immunohistochemical marker allows a reliable distinction. Recently, the over-expression of Wilms' tumor gene product WT1 was reported in astrocytic tumor cells. However, no sufficient data on WT1 expression in normal or reactive astrocytes are available. Therefore, we investigated WT1 expression in paraffin-embedded brain sections from 28 controls, 48 cases with astrogliosis of various etiology and 219 astrocytomas [World Health Organization (WHO) grades I-IV] by immunohistochemistry. In normal brains and in astrogliosis, expression of WT1 was restricted to endothelial cells. In astrocytomas, WT1-positive tumor cells were found in pilocytic astrocytomas (66.7% of cases), diffuse astrocytomas (52.7%) WHO grade II (52.7%), anaplastic astrocytomas (83.4%) and glioblastomas (98.1%). Overall, the majority of all astrocytic neoplasms (84.5%) expressed WT1. Establishing a cut-off value of 0% immunoreactive tumor cells served to recognize neoplastic astrocytes with 100% specificity and 68% sensitivity and was associated with positive and negative predictive values of 1 and 0.68, respectively. Therefore, WT1 expression in astrocytes indicates a neoplastic origin and might represent an important diagnostic tool to differentiate reactive from neoplastic astrocytes by immunohistochemistry.
Figures
Similar articles
-
WT1 Clone 6F-H2 Cytoplasmic Expression Differentiates Astrocytic Tumors from Astrogliosis and Associates with Tumor Grade, Histopathology, IDH1 Status, Apoptotic and Proliferative Indices: A Tissue Microarray Study.Asian Pac J Cancer Prev. 2020 Aug 1;21(8):2403-2413. doi: 10.31557/APJCP.2020.21.8.2403. Asian Pac J Cancer Prev. 2020. PMID: 32856872 Free PMC article.
-
WT1 in astrocytomas: Comprehensive evaluation of immunohistochemical expression and its potential utility in different histological grades.Indian J Cancer. 2019 Jul-Sep;56(3):197-201. doi: 10.4103/ijc.IJC_51_18. Indian J Cancer. 2019. PMID: 31389380
-
J1-31 protein expression in astrocytes and astrocytomas.Neuropathology. 2009 Oct;29(5):521-7. doi: 10.1111/j.1440-1789.2008.00979.x. Epub 2008 Nov 19. Neuropathology. 2009. PMID: 19019178
-
Proteins of the intermediate filament cytoskeleton as markers for astrocytes and human astrocytomas.Mol Chem Neuropathol. 1994 Feb-Apr;21(2-3):155-76. doi: 10.1007/BF02815349. Mol Chem Neuropathol. 1994. PMID: 7522006 Review.
-
Gliosis versus glioma?: don't grade until you know.Adv Anat Pathol. 2012 Jul;19(4):239-49. doi: 10.1097/PAP.0b013e31825c6a04. Adv Anat Pathol. 2012. PMID: 22692287 Review.
Cited by
-
Deciphering the Dialogue between Brain Tumors, Neurons, and Astrocytes.Am J Pathol. 2025 Jul;195(7):1193-1208. doi: 10.1016/j.ajpath.2025.04.013. Epub 2025 May 7. Am J Pathol. 2025. PMID: 40345526 Free PMC article. Review.
-
Neurofibromatosis-1 regulates neuroglial progenitor proliferation and glial differentiation in a brain region-specific manner.Genes Dev. 2010 Oct 15;24(20):2317-29. doi: 10.1101/gad.1957110. Epub 2010 Sep 28. Genes Dev. 2010. PMID: 20876733 Free PMC article.
-
WT1 is not a reliable marker to distinguish reactive from neoplastic astrocyte populations in the central nervous system.Brain Pathol. 2010 Nov;20(6):1090-5. doi: 10.1111/j.1750-3639.2010.00415.x. Epub 2010 Jun 22. Brain Pathol. 2010. PMID: 20576027 Free PMC article.
-
WT1/EGR1-mediated control of STIM1 expression and function in cancer cells.Front Biosci (Landmark Ed). 2011 Jun 1;16(7):2402-15. doi: 10.2741/3862. Front Biosci (Landmark Ed). 2011. PMID: 21622185 Free PMC article. Review.
-
WT1 Clone 6F-H2 Cytoplasmic Expression Differentiates Astrocytic Tumors from Astrogliosis and Associates with Tumor Grade, Histopathology, IDH1 Status, Apoptotic and Proliferative Indices: A Tissue Microarray Study.Asian Pac J Cancer Prev. 2020 Aug 1;21(8):2403-2413. doi: 10.31557/APJCP.2020.21.8.2403. Asian Pac J Cancer Prev. 2020. PMID: 32856872 Free PMC article.
References
-
- Agapova OA, Ricard CS, Salvador‐Silva M, Yang P, Hernandez MR (2001) Expression of matrix metalloproteinases and tissue inhibitors of metalloproteinases in human optic nerve head astrocytes. Glia 33:205–216. - PubMed
-
- Aldape KD, Ballman K, Furth A, Buckner JC, Giannini C, Burger PC et al (2004) Immunohistochemical detection of EGFRvIII in high malignancy grade astrocytomas and evaluation of prognostic significance. J Neuropathol Exp Neurol 63:700–707. - PubMed
-
- Armstrong JF, Pritchard‐Jones K, Bickmore WA, Hastie ND, Bard JB (1993) The expression of the Wilms' tumour gene, WT1, in the developing mammalian embryo. Mech Dev 40:85–97. - PubMed
-
- Asano K, Kubo O, Tajika Y, Huang MC, Takakura K, Ebina K, Suzuki S (1997) Expression and role of cadherins in astrocytic tumors. Brain Tumor Pathol 14:27–33. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
