

Self evaluation of communication experiences after laryngeal cancer - a longitudinal questionnaire study in patients with laryngeal cancer
- PMID: 18371189
- PMCID: PMC2329650
- DOI: 10.1186/1471-2407-8-80
Self evaluation of communication experiences after laryngeal cancer - a longitudinal questionnaire study in patients with laryngeal cancer
Abstract
Background: Aim of this longitudinal study was to investigate the sensitivity to change of the Swedish Self Evaluation of Communication Experiences after Laryngeal Cancer questionnaire (the S-SECEL), addressing communication dysfunction in patients treated for laryngeal cancer. Previous studies have highlighted the need for more specific questionnaires for this purpose.
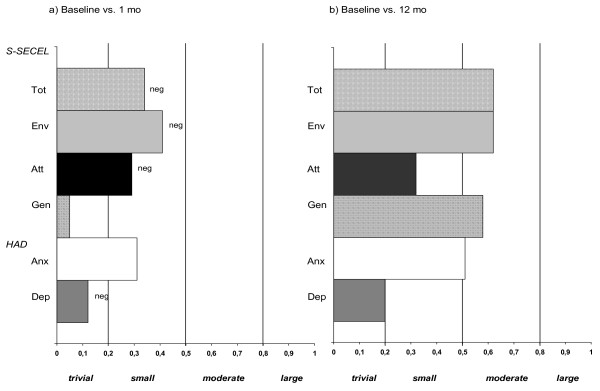
Methods: 100 patients with Tis-T4 laryngeal cancer were included prior to treatment onset. Patients answered four questionnaires at six occasions during one year; the S-SECEL, the European Organisation for Research and Treatment of Cancer (EORTC) Core Quality of Life Core Questionnaire (QLQ-C30) supplemented by the Head and Neck cancer module (QLQ-H&N35) and the Hospital Anxiety and Depression (HAD) scale. In addition, performance status was assessed. Differences within groups were tested with the Wilcoxon paired signed ranks test and between-group analyses were carried out using the Mann-Whitney U test. Magnitude of group differences was analyzed by means of effect sizes.
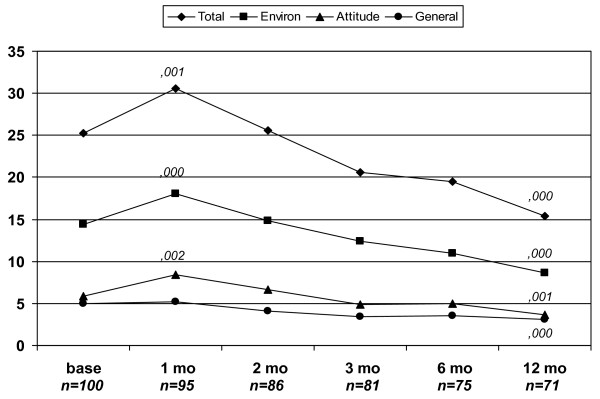
Results: The S-SECEL was well accepted with a response rate of 76%. Communication dysfunction increased at 1 month, followed by a continuous decrease throughout the year. Changes were statistically significant at most measurement, demonstrating the sensitivity of the S-SECEL to changes in communication over time. The S-SECEL and the EORTC QLQ-C30 with the QLQ-H&N35 demonstrated similar results; however the S-SECEL was more sensitive regarding communication dysfunction. The largest changes were found in the most diagnose specific items concerning voice and speech.
Conclusion: The S-SECEL was investigated in the largest Scandinavian longitudinal study concerning health-related quality of life (HRQL) in laryngeal cancer patients. The questionnaire was responsive to change and showed convergent results when compared to established HRQL questionnaires. Our findings also indicate that the S-SECEL could be a more suitable instrument than the EORTC QLQ-C30 with QLQ-H&N35 when measuring communication experiences in patients with laryngeal cancer; it is more sensitive, shorter and can be used on an individual basis. As a routine screening instrument the S-SECEL could be a valuable tool for identifying patients at risk for psychosocial problems and to help plan rehabilitation. It is therefore recommended for clinical use in evaluation of communication dysfunction for all patients with laryngeal cancer irrespective of treatment.
Figures
Similar articles
-
A longitudinal study of the Swedish Self-Evaluation of Communication Experiences after Laryngeal Cancer questionnaire in patients treated for laryngeal cancer.Acta Oncol. 2002;41(3):262-8. doi: 10.1080/02841860260088809. Acta Oncol. 2002. PMID: 12195745
-
Reliability and validity of the Italian self-evaluation of communication experiences after laryngeal cancer questionnaire.Head Neck. 2013 Nov;35(11):1606-15. doi: 10.1002/hed.23198. Epub 2012 Nov 20. Head Neck. 2013. PMID: 23169480
-
Self-evaluation of communication experiences after laryngectomy (SECEL): translation and psychometric properties in European Portuguese.Logoped Phoniatr Vocol. 2020 Jul;45(2):66-72. doi: 10.1080/14015439.2019.1615544. Epub 2019 May 20. Logoped Phoniatr Vocol. 2020. PMID: 31109211
-
Quality of life assessment in Hodgkin's disease: a new comprehensive approach. First experiences from the EORTC/GELA and GHSG trials. EORTC Lymphoma Cooperative Group. Groupe D'Etude des Lymphomes de L'Adulte and German Hodgkin Study Group.Ann Oncol. 1998;9 Suppl 5:S147-54. doi: 10.1093/annonc/9.suppl_5.s147. Ann Oncol. 1998. PMID: 9926255 Review.
-
Functional outcomes following treatment for advanced laryngeal cancer. Part I--Voice preservation in advanced laryngeal cancer. Part II--Laryngectomy rehabilitation: the state of the art in the VA System. Research Speech-Language Pathologists. Department of Veterans Affairs Laryngeal Cancer Study Group.Ann Otol Rhinol Laryngol Suppl. 1998 May;172:1-27. Ann Otol Rhinol Laryngol Suppl. 1998. PMID: 9597955 Review.
Cited by
-
Validation of the Swedish M. D. Anderson Dysphagia Inventory (MDADI) in patients with head and neck cancer and neurologic swallowing disturbances.Dysphagia. 2012 Sep;27(3):361-9. doi: 10.1007/s00455-011-9375-8. Epub 2011 Nov 22. Dysphagia. 2012. PMID: 22105944
-
The effect of a voucher incentive on a survey response rate in the clinical setting: a quasi-randomized controlled trial.BMC Med Res Methodol. 2018 Aug 16;18(1):86. doi: 10.1186/s12874-018-0544-4. BMC Med Res Methodol. 2018. PMID: 30115037 Free PMC article. Clinical Trial.
-
Psychological Distress and Quality of Life in Patients with Laryngeal Cancer: A Review.Healthcare (Basel). 2025 Jun 29;13(13):1552. doi: 10.3390/healthcare13131552. Healthcare (Basel). 2025. PMID: 40648576 Free PMC article. Review.
-
Effects of total laryngectomy on olfactory function, health-related quality of life, and communication: a 3-year follow-up study.BMC Ear Nose Throat Disord. 2009 Jul 29;9:8. doi: 10.1186/1472-6815-9-8. BMC Ear Nose Throat Disord. 2009. PMID: 19640307 Free PMC article.
-
Mental adjustment to cancer and its relation to anxiety, depression, HRQL and survival in patients with laryngeal cancer - a longitudinal study.BMC Cancer. 2011 Jun 30;11:283. doi: 10.1186/1471-2407-11-283. BMC Cancer. 2011. PMID: 21718478 Free PMC article.
References
-
- Bjordal K, Kaasa S, Mastekaasa A. Quality of life in patients treated for head and neck cancer: A follow-up study 7 to 11 years after radiotherapy. Int J Radiat Oncol Biol Phys. 1994;28:847–856. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
