

Relationships of thoracic aortic wall calcification to cardiovascular risk factors: the Multi-Ethnic Study of Atherosclerosis (MESA)
- PMID: 18371491
- PMCID: PMC2323597
- DOI: 10.1016/j.ahj.2007.11.019
Relationships of thoracic aortic wall calcification to cardiovascular risk factors: the Multi-Ethnic Study of Atherosclerosis (MESA)
Abstract
Background: The aim of this article is to determine the relationships between aortic wall calcification (AWC) including ascending and descending thoracic aortic calcification and sex, race/ethnicity, age, and traditional risk factors. Allison et al (Arterioscler Thromb Vasc Biol. 2004;24:331-336) previously described the relationship of noted risk factors and AWC as detected by computed tomography (CT) in smaller cohorts. We performed a cross-sectional study to determine which of these variables are independently associated with thoracic calcium.
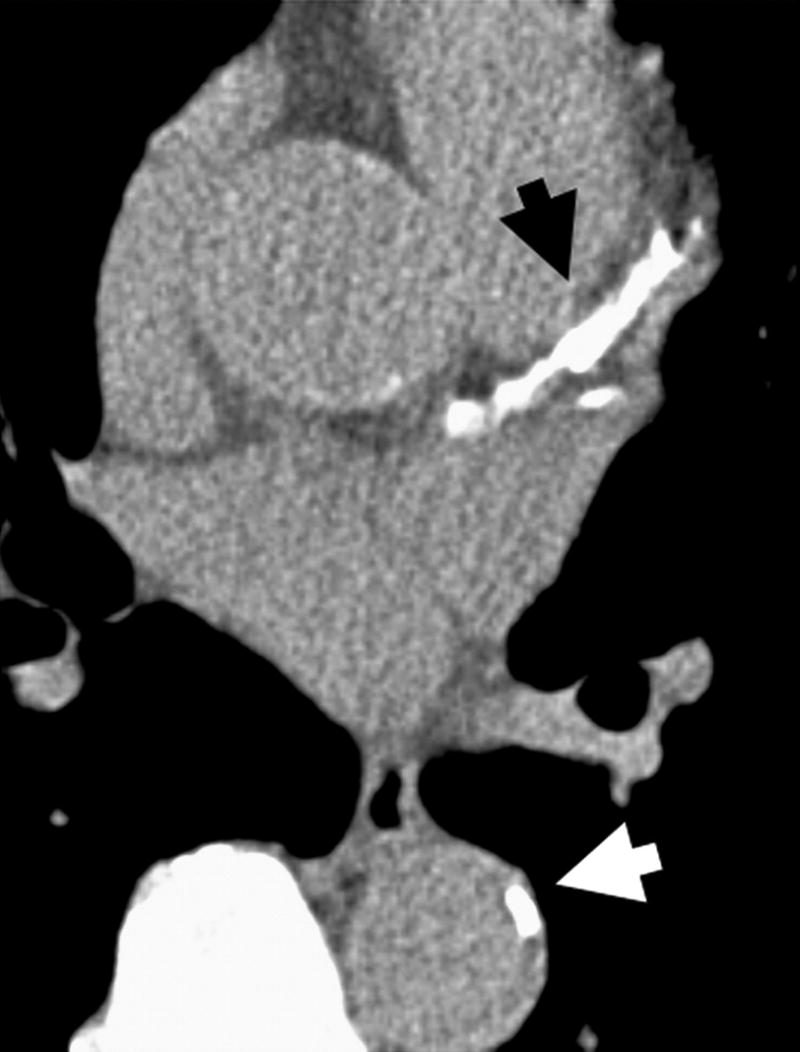
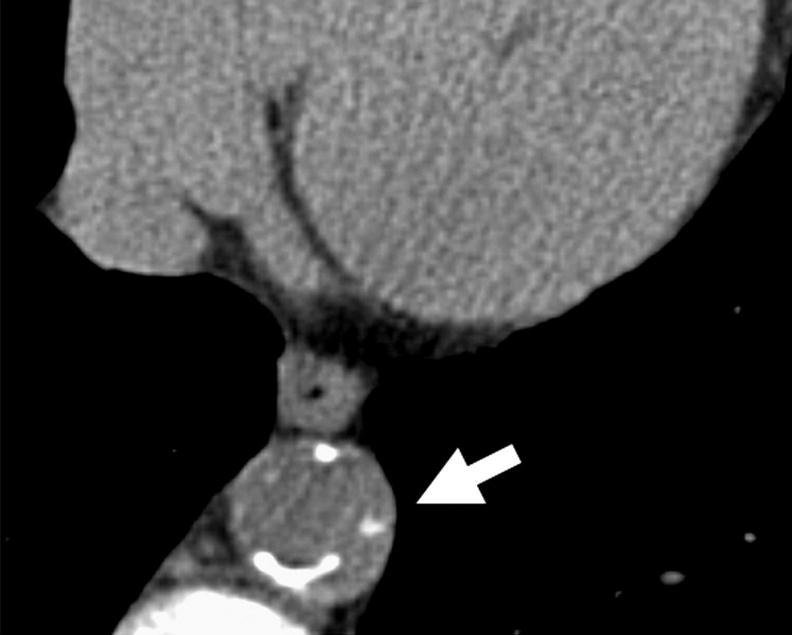
Methods: The MESA population included a population-based sample of 4 ethnic groups (12% Chinese, 38% white, 22% Hispanic, and 28% black) of 6814 women and men aged 45 to 84 years. Computed tomographic scans were performed for all participants. We quantified AWC, which ranged from the lower edge of the pulmonary artery bifurcation to the cardiac apex. Multivariable logistic regression was used to evaluate relationships between AWC and measured cardiovascular risk factors.
Results: Overall prevalence of AWC was 28.0%. In the ethnic groups, prevalence of AWC was 32.4% Chinese, 32.4% white, 24.9% Hispanic, and 22.4% black. All age categories of females had a higher prevalence of thoracic calcification than males (total age prevalence 29.1% and 26.8%, respectively). Aortic wall calcifications were most strongly associated with hypertension and current smoking. In addition, diabetes, hypercholesterolemia, high level of low-density lipoprotein, low level of high-density lipoprotein, family history of myocardial infarction , and high C-reactive protein were all associated with increased AWC. Overall P value for difference between sexes for prevalence of AWC is 0.037. Overall P value for difference between race for prevalence of AWC is <.001. The only significant sex differences distributed by race were for Chinese (P = .035) and Hispanic (P = .042) participants.
Conclusions: Risk factors for aortic calcification were similar to cardiovascular risk factors in a large population-based cohort. Surprisingly, AWC was similar for the Chinese and white populations despite the fact that MESA demonstrated that coronary calcium was more prevalent in the white population. Further studies are needed to investigate whether aortic calcification is a risk factor for coronary disease, independent of coronary calcification.
Figures
References
-
- Thom T, Haase N, Rosamond W, Howard VJ, Rumsfeld J, Manolio T, Zheng ZJ, Flegal K, O’Donnell C, Kittner S, Lloyd-Jones D, Goff DC, Jr, Hong Y, Adams R, Friday G, Furie K, Gorelick P, Kissela B, Marler J, Meigs J, Roger V, Sidney S, Sorlie P, Steinberger J, Wasserthiel-Smoller S, Wilson M, Wolf P. Heart disease and stroke statistics--2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2006;113:e85–151. - PubMed
-
- Stary HC, Chandler AB, Dinsmore RE, Fuster V, Glagov S, Insull W, Jr, Rosenfeld ME, Schwartz CJ, Wagner WD, Wissler RW. A definition of advanced types of atherosclerotic lesions and a histological classification of atherosclerosis. A report from the Committee on Vascular Lesions of the Council on Arteriosclerosis, American Heart Association. Circulation. 1995;92:1355–74. - PubMed
-
- Witteman JC, Kannel WB, Wolf PA, Grobbee DE, Hofman A, D’Agostino RB, Cobb JC. Aortic calcified plaques and cardiovascular disease (the Framingham Study) Am J Cardiol. 1990;66:1060–1064. - PubMed
-
- Witteman JC, Kok FJ, van Saase JL, Valkenburg HA. Aortic calcification as a predictor of cardiovascular mortality. Lancet. 1986;2:1120–1122. - PubMed
-
- Hollander M, Hak AE, Koudstaal PJ, Bots ML, Grobbee DE, Hofman A, Witteman JC, Breteler MM. Comparison between measures of atherosclerosis and risk of stroke: the Rotterdam Study. Stroke. 2003 Oct;34:2367–2372. - PubMed
Publication types
MeSH terms
Grants and funding
- R01-HL-071739/HL/NHLBI NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01-HC-95163/HC/NHLBI NIH HHS/United States
- N01-HC-95159/HC/NHLBI NIH HHS/United States
- N01-HC-95165/HC/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- R01 HL063963/HL/NHLBI NIH HHS/United States
- N01-HC-95160/HC/NHLBI NIH HHS/United States
- N01-HC-95161/HC/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- R01 HL071739/HL/NHLBI NIH HHS/United States
- N01-HC-95162/HC/NHLBI NIH HHS/United States
- N01-HC-95169/HC/NHLBI NIH HHS/United States
- N01-HC-95164/HC/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous
