

Control of a hospital-wide vancomycin-resistant Enterococci outbreak
- PMID: 18371517
- PMCID: PMC7115253
- DOI: 10.1016/j.ajic.2007.06.005
Control of a hospital-wide vancomycin-resistant Enterococci outbreak
Abstract
Background: To analyze control measures used to eradicate a large vancomycin-resistant Enterococci (VRE) outbreak in a nonendemic 1600-bed tertiary care institution.
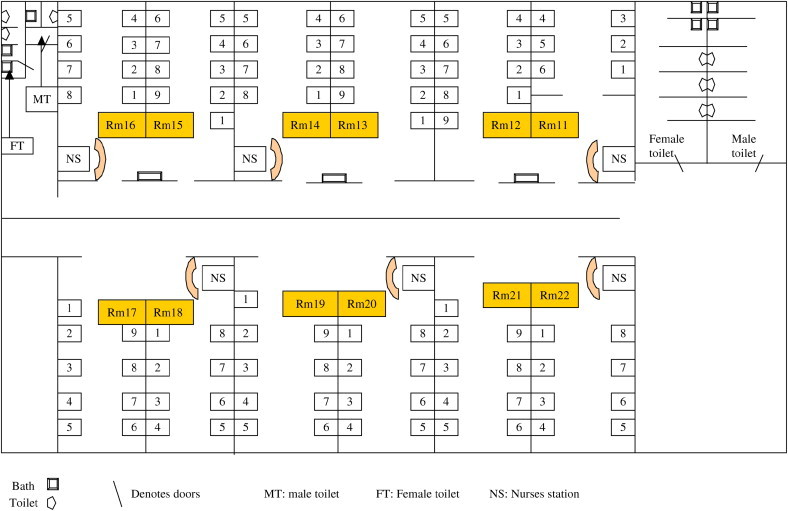
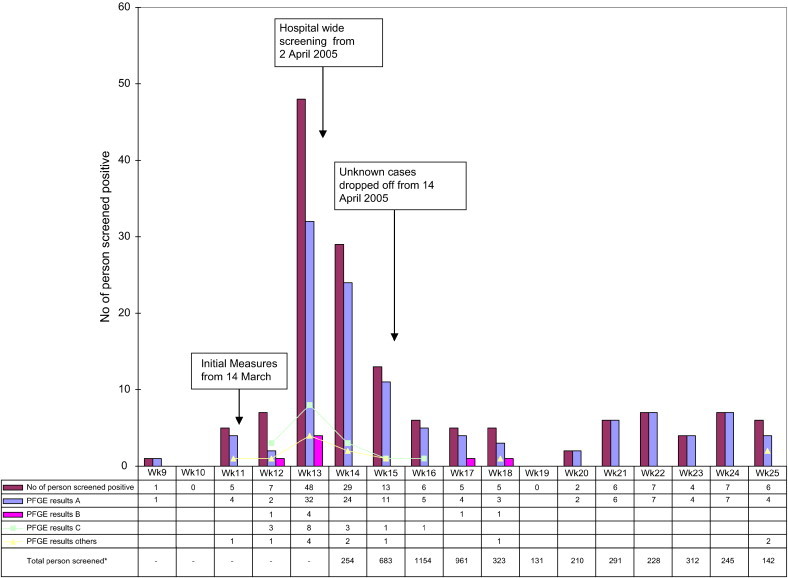
Methods: In mid-March 2005, VRE Van B was isolated from 2 clinical samples from different wards. Despite such measures as screening patients sharing rooms with index cases and isolating VRE patients, 43 isolates from different wards were detected by the end of March 2005. To eradicate a hospital-wide outbreak, a coordinated strategy between March and June 2005 comprised (1) formation of a VRE task force, (2) hospital-wide screening, (3) isolation of carriers, (4) physical segregation of contacts, (5) surveillance of high-risk groups, (6) increased cleaning, (7) electronic tagging of VRE status, and (8) education and audits. This is a retrospective study of this multipronged approach to containing VRE. The adequacy of rectal swab sampling for VRE was assessed in a substudy of 111 patients. The prevalence of methicillin-resistant Staphylococcus aureus (MRSA)/VRE co-colonization or co-infection also was determined.
Results: A total of 19,574 contacts were identified. Between April and June 2005, 5095 patients were screened, yielding 104 VRE carriers, 54 of whom (52%) were detected in the first 2 weeks of hospital-wide screening. The initial positive yield of 11.4% of persons actively screened declined to 4.2% by the end of June 2005. Pulsed-field typing revealed 1 major clone and several minor clones among the 151 total VRE cases, including 4 clinical cases. Hospital-wide physical segregation of contacts from other patients was difficult to achieve in communal wards. Co-colonization or co-infection with MRSA, which was present in 52 of 151 cases (34%) and the indefinite electronic tagging of positive VRE status strained limited isolation beds. Analysis of 2 fecal or rectal specimens collected 1 day apart may detect at least 83% of VRE carriers.
Conclusion: A multipronged strategy orchestrated by a central task force curbed but could not eradicate VRE. Control measures were confounded by hospital infrastructure and high MRSA endemicity.
Figures
References
-
- Chlebicki MP, Ling ML, Koh TH, Hsu LY, Tan BH, How KB, et al. National Nosocomial Infections Surveillance (NNIS) system report: data summary from January 1992-April 2000, issued June 2000. Am J Infect Control. 2000;28:429–448. - PubMed
-
- Chlebicki M.P., Ling M.L., Koh T.H. First outbreak of vancomycin-resistant Enterococcus faecium in a tertiary-care hospital in Singapore. Infect Cont Hosp Epidemiol. 2006;27:991–993. - PubMed
-
- Christiansen K.J., Tibbett P.A., Beresford W. Eradication of a large outbreak of a single strain of vanB vancomycin-resistant Enterococcus faecium at a major Australian teaching hospital. Infect Control Hosp Epidemiol. 2004;25:384–390. - PubMed
-
- National Committee for Clinical Laboratory Standards . National Committee for Clinical Laboratory Standards; Wayne (PA): 2002. Performance standards for antimicrobial susceptibility testing: twelfth informational supplement.
-
- Oon L.L., Ling M.L., Chiew Y.F. Gastrointestinal colonisation of vancomycin-resistant Enterococcus in a Singapore teaching hospital. Pathology. 2001;33:216–221. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
