

Intra-arterial nimodipine for severe cerebral vasospasm after aneurysmal subarachnoid hemorrhage: influence on clinical course and cerebral perfusion
- PMID: 18372422
- PMCID: PMC8118836
- DOI: 10.3174/ajnr.A1005
Intra-arterial nimodipine for severe cerebral vasospasm after aneurysmal subarachnoid hemorrhage: influence on clinical course and cerebral perfusion
Abstract
Background and purpose: The efficacy of intra-arterial administration of nimodipine (IAN) in patients with severe vasospasm after aneurysmal subarachnoid hemorrhage (SAH) remains unproved. The goal of the present study was to investigate the clinical effect and cerebral perfusion after IAN in patients with severe vasospasm refractory to hemodynamic treatment.
Materials and methods: Twenty-six of 214 patients with aneurysmal SAH were included in the prospective study, approved by the local ethics committee. All patients met the criteria of medically refractory cerebral vasospasm. Effectiveness was monitored angiographically by digital subtraction angiography and by transcranial Doppler (TCD), perfusion CT (PCT), and neurologic examination during treatment course and follow-up.
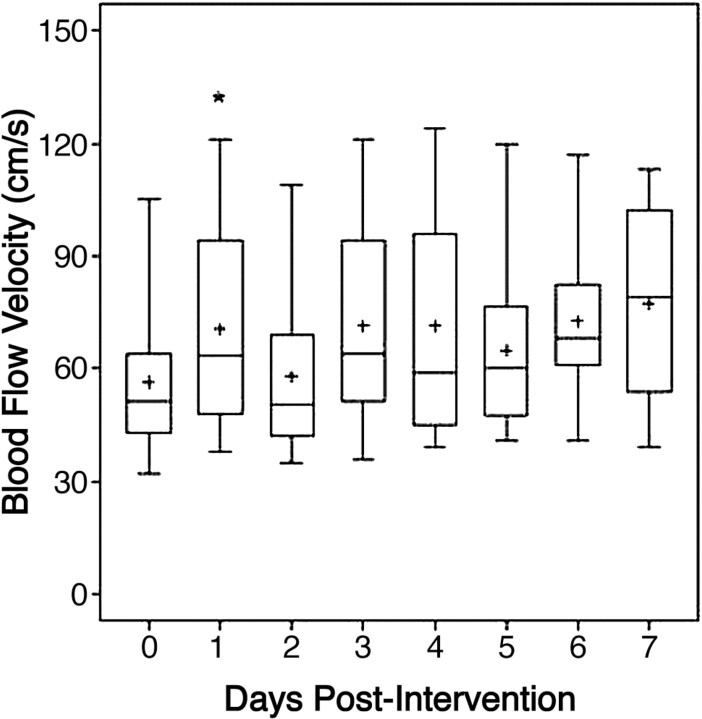
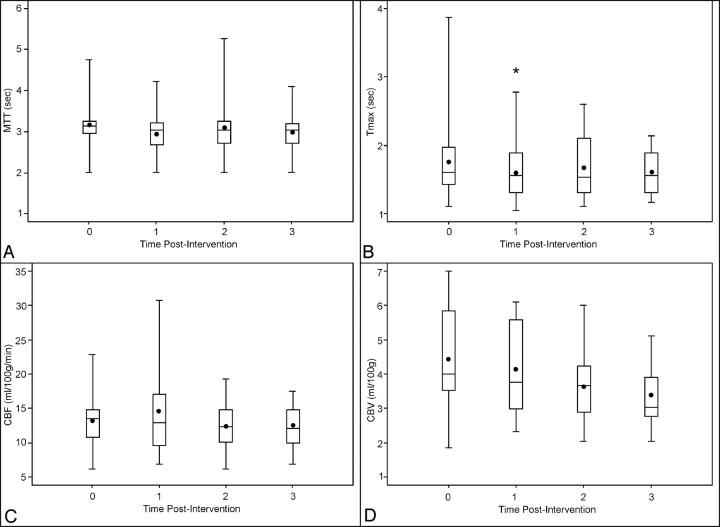
Results: No angiographic effect was observed in 8 patients. The pooled PCT values revealed a reduction of time to peak (P = .03) and mean transit time (P = .17) 1 day after intervention. This effect did not persist during the following days. The pooled TCD analysis demonstrated a transient increase in flow 1 day after intervention (P = .03). No trend was evident during the next 7 days after intervention. Additional infarction was experienced by 61.1% of patients.
Conclusions: IAN in a selective patient group resulted in a positive response with reduction of angiographic vasospasm and increase in cerebral perfusion as detected by PCT after 24 hours. Therefore, IAN appears more effective than intra-arterial papaverine. Nevertheless the efficacy of IAN is temporary. Therefore, the search for more effective treatment strategies to reduce critical vasospasm and to improve cerebral perfusion must be continued.
Figures
Similar articles
-
Feasibility and safety of intrathecal nimodipine on posthaemorrhagic cerebral vasospasm refractory to medical and endovascular therapy.Clin Neurol Neurosurg. 2008 Sep;110(8):784-90. doi: 10.1016/j.clineuro.2008.05.001. Epub 2008 Jun 12. Clin Neurol Neurosurg. 2008. PMID: 18554777
-
Intra-arterial nimodipine for cerebral vasospasm after subarachnoid haemorrhage: Influence on clinical course and predictors of clinical outcome.Neuroradiol J. 2016 Feb;29(1):72-81. doi: 10.1177/1971400915626429. Epub 2016 Jan 29. Neuroradiol J. 2016. PMID: 26825134 Free PMC article.
-
Continuous selective intra-arterial application of nimodipine in refractory cerebral vasospasm due to aneurysmal subarachnoid hemorrhage.Biomed Res Int. 2014;2014:970741. doi: 10.1155/2014/970741. Epub 2014 Jan 16. Biomed Res Int. 2014. PMID: 24527461 Free PMC article.
-
Intra-arterial papaverine infusions for the treatment of cerebral vasospasm induced by aneurysmal subarachnoid hemorrhage.Neurocrit Care. 2005;2(2):124-32. doi: 10.1385/NCC:2:2:124. Neurocrit Care. 2005. PMID: 16159054 Review.
-
Effectiveness of intrathecal nicardipine on cerebral vasospasm in non-traumatic subarachnoid hemorrhage: a systematic review.JBI Database System Rev Implement Rep. 2018 Oct;16(10):2013-2026. doi: 10.11124/JBISRIR-2017-003493. JBI Database System Rev Implement Rep. 2018. PMID: 30335041
Cited by
-
Vasogenic edema of the Basal Ganglia after intra-arterial administration of nimodipine for treatment of vasospasm.J Korean Neurosurg Soc. 2011 Feb;49(2):112-5. doi: 10.3340/jkns.2011.49.2.112. Epub 2011 Feb 28. J Korean Neurosurg Soc. 2011. PMID: 21519500 Free PMC article.
-
Treatment of cerebral vasospasm following aneurysmal subarachnoid haemorrhage: a systematic review and meta-analysis.Eur Radiol. 2017 Aug;27(8):3333-3342. doi: 10.1007/s00330-016-4702-y. Epub 2016 Dec 21. Eur Radiol. 2017. PMID: 28004163
-
Duration of Vasodilatory Action After Intra-arterial Infusions of Calcium Channel Blockers in Animal Model of Cerebral Vasospasm.Neurocrit Care. 2021 Jun;34(3):867-875. doi: 10.1007/s12028-020-01112-0. Epub 2020 Sep 25. Neurocrit Care. 2021. PMID: 32978731
-
An L-type calcium channel blocker nimodipine exerts anti-fibrotic effects by attenuating TGF-β1 induced calcium response in an in vitro model of thyroid eye disease.Eye Vis (Lond). 2024 Sep 6;11(1):37. doi: 10.1186/s40662-024-00401-5. Eye Vis (Lond). 2024. PMID: 39237996 Free PMC article.
-
Continuous selective intraarterial infusion of nimodipine for therapy of refractory cerebral vasospasm.Neurocrit Care. 2010 Jun;12(3):346-51. doi: 10.1007/s12028-009-9317-6. Neurocrit Care. 2010. PMID: 20033353
References
-
- Findlay JM, Deagle GM. Causes of morbidity and mortality following intracranial aneurysm rupture. Can J Neurol Sci 1998;25:209–15 - PubMed
-
- Kassell NF, Torner JC, Haley EC Jr, et al. The International Cooperative Study on the Timing of Aneurysm Surgery. Part 1. Overall management results. J Neurosurg 1990;73:18–36 - PubMed
-
- Kassell NF, Torner JC, Jane JA, et al. The International Cooperative Study on the Timing of Aneurysm Surgery. Part 2. Surgical results. J Neurosurg 1990;73:37–47 - PubMed
-
- Rabinstein AA, Pichelmann MA, Friedman JA, et al. Symptomatic vasospasm and outcomes following aneurysmal subarachnoid hemorrhage: a comparison between surgical repair and endovascular coil occlusion. J Neurosurg 2003;98:319–25 - PubMed
-
- Barker FG 2nd, Ogilvy CS. Efficacy of prophylactic nimodipine for delayed ischemic deficit after subarachnoid hemorrhage: a metaanalysis. J Neurosurg 1996;84:405–14 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous